






Introduction
Different shapes of the acromion are associated with a variety of pathologies such as impingement syndrome and rotator cuff tear (RCT) [1]. Rotator cuff tears are one of the most common disorders of the shoulder, with recent studies emphasising the specific acromion morphologies predisposing to it. Although the specific aetiology of RCT is not fully known, it has been proposed that it results from a combination of intrinsic and extrinsic factors. The degenerative changes, hypovascularity, and micro structural collagen fibre abnormalities are the most important intrinsic factors. And the considerable extrinsic factors include subacromial impingement with chronic repetitive use and tensile overload [2]. In 1983, Neer stated that 95% of cuff tears are caused by mechanical impingement which was successfully treated by anterior acromioplasty [3]. Hence, acromioplasty proves to be the standard operative treatment for impingement lesions with a substantial increase in its incidence [4]. The accurate assessment of the extrinsic factors results in better management of the patients.
Henceforth, several classifications of the acromial morphology have been proposed, including Bigliani et al. (1986) and Kitay et al. (1995) describing the acromial slope (AS); furthermore, Kitay et al. (1995) and Aoki et al. (1986) described the acromial tilt [5-7].
Other studies include one by Banas et al., who described the types of frontal plane slope of the acromion on magnetic resonance imaging (MRI) and found a lower lateral acromial angle (LAA) in patients with rotator cuff disease [8]. Similarly, Nyffeler et al. observed that the acromion of patients with more lateral extension had higher incidence of rotator cuff tear, and they also described the acromion index (AI) in their study [9].
In order to advance our understanding of rotator cuff disease, further investigation of the radiographic characteristics of the acromion and their potential relationships to rotator cuff disease is needed. The role of the acromion is still ambiguous, although several studies have attempted to correlate Neer’s original theory of extrinsic mechanical impingement as the primary aetiological factor of rotator cuff disease. MRI has proven to be a single solution both for characterising acromial morphology and for evaluating rotator cuff tears. In this study we evaluated six commonly used parameters of acromial morphology (acromial type, acromial thickness, critical shoulder angle, lateral acromial angle, acromiohumeral distance, and acromion index) and their relationship to rotator cuff tears.
Material and methods
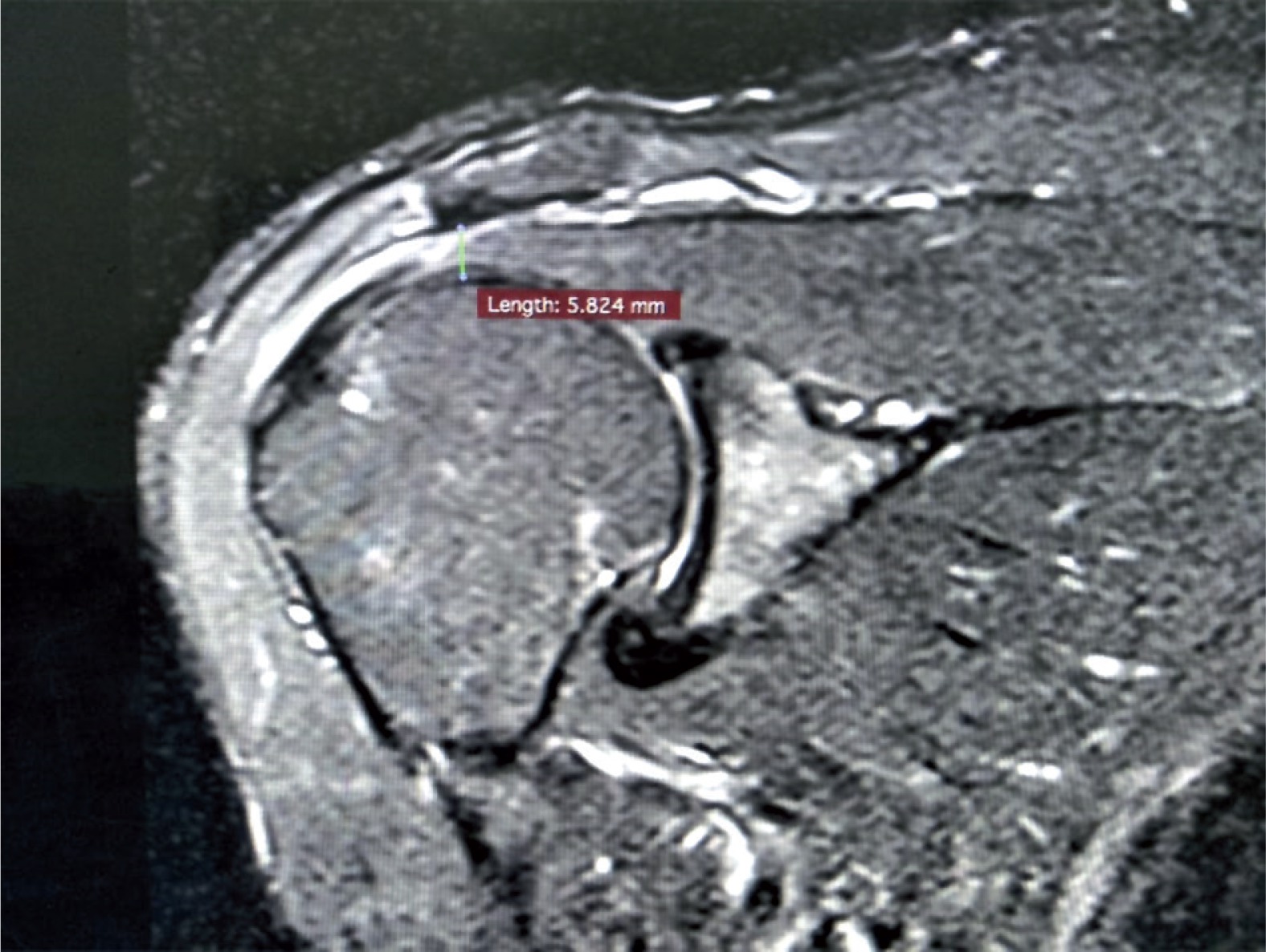
This study was carried out in the period from January 2015 to August 2017 in our institution and included 68 patients with RCT, either partial or full thickness (patient group). In addition, 30 subjects with an intact rotator cuff on the asymptomatic side were recruited to serve as a control group. The exclusion criteria included previous surgery, fractures and/or dislocation, infections or tumours of the shoulder, and cases with acromial spurs. All patients were imaged with MRI according to their side of complaint by a single technician, and acromial measurements were taken by a single radiologist. In order to study the incidence of each acromial shape, 30 age- and sex-matched patients without RCT were included as the control group. From a retrospective study of 98 patients, we measured acromial type (Bigliani) and acromial thickness (AT) measured on sagittal oblique images just lateral to the acromioclavicular joint as the widest part of acromion in plane perpendicular to the long axis of acromion; acromiohumeral distance (AHD) refers to the shortest distance between line parallel to the inferior edge of acromion and parallel tangent to the superior part of humeral head (as shown in Figure 1).
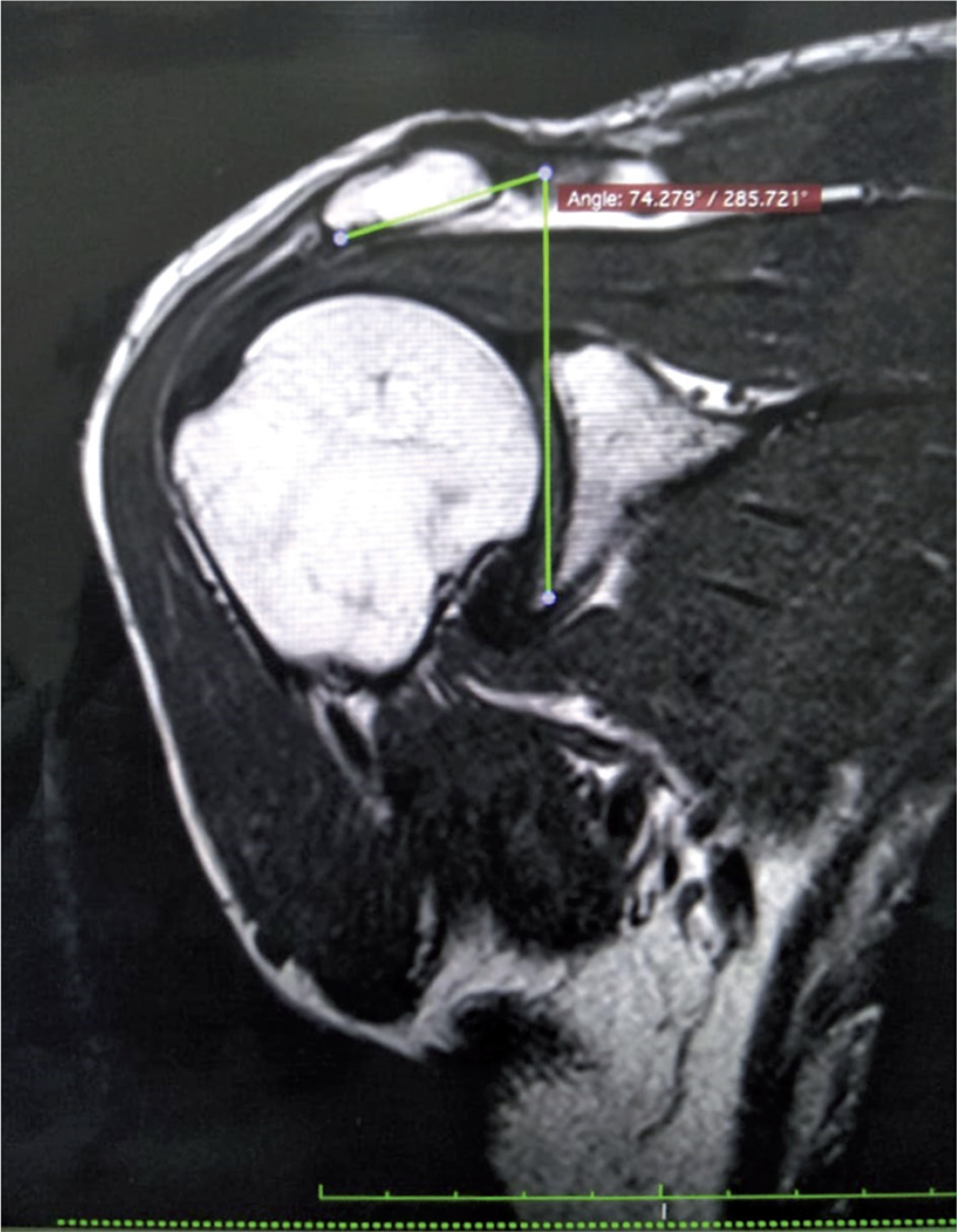
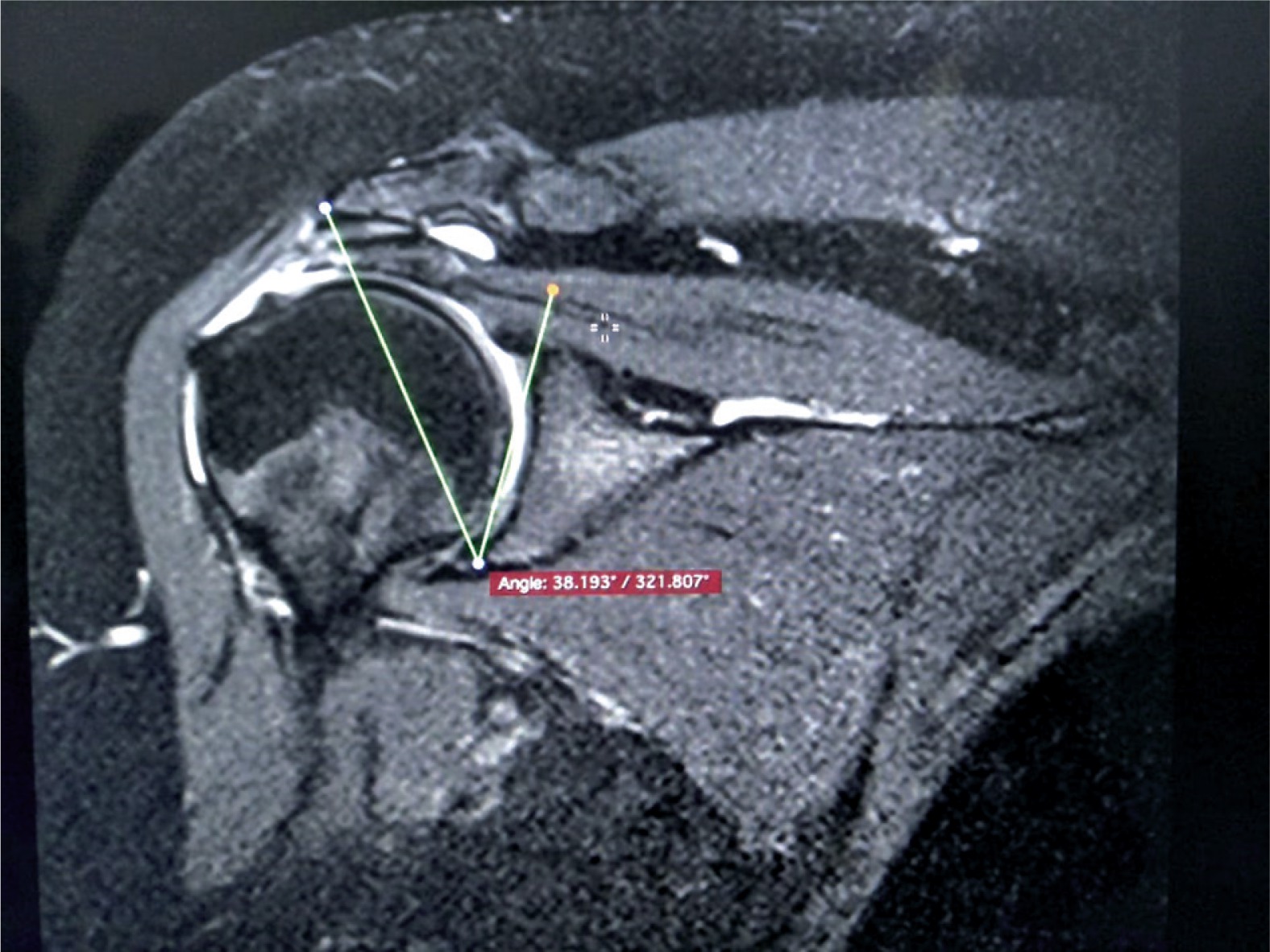
LAA was measured from an oblique coronal MRI slice just posterior to the acromioclavicular joint. The angle was determined by the intersection of a line parallel to the acromion undersurface and a second line parallel to the glenoid fossa (as shown in Figure 2). The critical shoulder angle (CSA) is measured between a line through the inferior lateral edge of the glenoid to the inferior lateral edge of the acromion and a line parallel to the glenoid (as shown in Figure 3) and the AI. The AI (A/B) is calculated by dividing the distance between the osseous glenoid plane to the lateral border of the acromion (A) by the distance between the osseous glenoid plane and the most lateral part of the proximal humerus, from 68 patients with partial or full-thickness supraspinatus tendon tears and 30 controls without subacromial pathology (as shown in Table 1 of the descriptive statistics). Later we evaluated these parameters and their relationship with RCT. All MRI images of our study were performed by using a 1.5-Tesla unit system (Siemens). A dedicated shoulder array coil was used. When imaging the shoulder with MRI, patients were placed in a supine position with their arms at the sides of their body in partial external rotation with the shoulder coil. Initially, localiser images were obtained, followed by coronal oblique, sagittal oblique, and axial images. The coronal oblique plane was selected parallel to the course of the supraspinatus tendon itself for optimal visualisation of the tendon.
Table 1
Descriptive statistics
Official permission to carry out the study was obtained from the local medical research Ethics Committee. Written, informed consent was obtained from all study participants.
Results
Of 68 patients with rotator cuff tear, supraspinatus was the most common pathological tendon, with 86% (59) of cases showing abnormalities. The average age of the patients was 45.11 ± 21.45 years with male dominance (80%). Partial tears of rotator cuff were more common than complete tears. Forty-eight cases showed partial tears in supraspinatus as compared to 11 cases of complete tears. The acromial type and acromial slope did not show any correlation with any particular cuff lesion (as shown in Table 2). AT and AI of controls were significantly smaller than cuff-tear patients. The LAAs of cuff-tear patients differed significantly from those of control patients. The mean acromial thickness in patients with RCT in our study was 8.5 mm.
Table 2
Acromial types in different groups
| Acromial type | Control group, n = 30 | Partial RCT, n = 57 | Complete RCT, n = 11 |
|---|---|---|---|
| Type I (flat) | 4 | 5 | 0 |
| Type II (curved) | 19 | 29 | 5 |
| Type III (hooked) | 6 | 21 | 5 |
| Type IV (convex) | 1 | 2 | 1 |
The impingement patients demonstrated significantly greater acromial thickness, larger CSA and decreased AHD, and decreased LAA compared to their control counterparts (as shown in Table 3).
Table 3
Comparison of acromial type II and type III in rotator cuff tears (partial and complete) with control group regarding acromial measurements
Discussion
Identifying the presence of bony impingement of the subacromial space may aid in a better understanding of predispositions to RC pathology. The factors affecting this space are the type of acromion, which was classified by Bigliani as three types, and later a fourth type was updated. They include type 1 – flat, type II – curved, and type III – hooked acromion morphology, and more recently type IV – convex morphology was added (Table 2) [2].
In the present study, the mean acromion thickness in patients with RCT was significantly thicker than in the control group (p = 0.002). This is in accordance with the conclusion of previous studies [10,11]; however, there is a slight difference regarding the mean acromial thickness in patients with RCT. It was 8.8 mm in the study by Paraskevas et al. [10] and 8.3 mm in the study of Oh et al. [11], but in our study it was 8.5 mm, favouring the previous studies. The presence of os acromiale also decreases the volume of the sub-acromial space and may result in impingement syndromes in some cases. Os acromiale is commonly unilateral and more frequent in type III acromial shape. Detection of the os acromiale on MR images is best achieved by using the axial sequence that includes the acromion [12].
Many studies, which reported no difference in the acromial index of patients who had calcifying tendinitis, partial-thickness rotator cuff tears, or full-thickness rotator cuff tears, called into question the biomechanical theory proposed by Nyffeler et al. regarding the association between large acromial index and rotator cuff disease as well as between small acromial index and osteoarthritis [9,13,14]. In contrast, our study supported Nyffeler et al. because a high AI index was seen in RCT patients, especially for full thickness tears [9]. Torrens et al. also reported similar findings in a study in Spain, in which patients with rotator cuff tears had a significantly larger acromial index of 0.72 compared with 0.68 in patients without cuff pathology, and there were differences between the sexes [15]. It was observed that high AI can be one of the associated factors for progression of severity of rotator cuff tears.
One of the other important parameters measured in our study was lateral acromial angle (LAA) on coronal oblique images. In our study, as well as in another by Banas et al., it was found that an extremely low LAA of less than 70° only occurs in cuff tears. Banas et al. reported that eight patients with complete tears had LAA of less than 70° and an average age of 54 years, whereas the average age of the remaining 18 patients with cuff tears and LAA greater than 70° was 70 years [8]. Hence the LAA showed fair correlation with age in our study, and there was moderate correlation (PCC = 0.46) in the original study by Banas et al. In our opinion, the LAA can help differentiate, on the one hand, between controls and rotator cuff tears and, on the other hand, between impingement and rotator cuff tears.
In our study CSA was found to be 34.6, corroborating with several other authors, such as Gerber et al., Spiegl et al., Moor et al., and Bouaicha et al., who also found similar results [16-19]. Gerber et al. demonstrated a biomechanical study that a high CSA may induce overload of the supraspinatus tendon, particularly at low degrees of active abduction [16]. Garcia et al., in a retrospective study, made a postoperative ultrasound examination after arthroscopic repair of RCTs and found that higher CSA significantly increased the risk of a full thickness rotator cuff re-tear after arthroscopic repair [20]. Although for Kirsch et al. CSA is a strong radiographic predictor of rotator cuff pathology, it did not have a predictive effect on outcomes after arthroscopic repair of atraumatic full-thickness tears [21].
Weiner and Macnab observed that AHD less than 7 mm is considered proof of a full-thickness tear of the supraspinatus tendon in more than 90% of cases [22].
Werner et al. believed that the cut-off point for AHD on MRI should be ≤ 6 mm, i.e. lower than on conventional radiograph [23]. In our study the AHD was found to be significantly smaller than in the control group. The present study found a mean subacromial space measurement of 7.71 mm in the control group, which does not corroborate with the findings of Werner et al., and 6.87 mm in patients with rotator cuff injuries, favouring many other studies [24-26].
AT, AHD, AI, and LAA were compared between each of the four acromial types in patients with RCT and the control group, and we found that all these acromial measurements were significantly different between only type III acromial shape and the control group. Hence, it could be proposed that it is significantly associated with increased risk of RCT. Paraskevas et al. also studied the clinical significance of the shape of the anterior third of acromion in relation to the impingement syndrome as well as to RCT [10].
Conclusions
Type 3 acromion is most commonly associated with RCT. The probability of RCT increases if AT > 8.5 mm, LAA < 70°, AI > 0.7, CSA > 35°, and AHD < 7 mm. A better defined acromial morphological criteria should be structured, containing a scoring system from which risk of RCT can be anticipated.