






Introduction
The problem of an insufficient number of physicians is growing all over Europe. One of the specialties that is greatly affected by medical staff shortages is radiology. The main reason is an increasing number of imaging studies, especially computed tomography (CT) and magnetic resonance imaging (MRI) in healthcare; e.g., in one of the centres in Poland the number of CT studies doubled between 2010 and 2020 [1]. Another cause involves the growing role of imaging modalities in medical management protocols; e.g., oncological management requires follow-up imaging of several body regions several times per year, and in multiple sclerosis patients follow-up MRI studies are mandatory and usually performed once a year [2,3]. Another factor is associated with the increasing age of populations in developed countries, as older people need more imaging examinations.
The process of training radiologists is not fast enough to cover the needs of reporting the growing number of imaging studies. The shortage of radiologists is especially severe in small towns and the countryside. In the past, it was partially solved by radiologists from the larger cities who travelled to smaller centres once or twice a week to report the imaging studies. However, nowadays this solution is not sufficient, because the shortages of radiologists also affect big cities.
Digitalization of imaging studies (including plain radiography) and the development of Picture Archiving and Communication Systems (PACS) have enabled the transfer of images via the Internet. Thus, imaging studies can be assessed and reports written anywhere in the world (teleradiology). Therefore, teleradiology potentially solves the problem of radiologist shortages in areas with very low numbers of radiologists. In fact, teleradiology is one of the most rapidly developing fields of telemedicine. However, there are many organizational, technical, and legal issues that should be taken into account in the application of teleradiology systems, which will be discussed below.
Right to healthcare – international provisions
The right to health is frequently listed among the basic human rights. It appeared in the United Nations’ International Covenant on Economic, Social, and Cultural Rights of 1966. Therein, art. 12 stated that “The States Parties to the present Covenant recognize the right of everyone to the enjoyment of the highest attainable standard of physical and mental health” [4]. In the European Union’s Charter of Fundamental Rights, developed and approved over 3 decades later, the wording is much more detailed: “Everyone has the right of access to preventive health care and the right to benefit from medical treatment under the conditions established by national laws and practices. A high level of human health protection shall be ensured in the definition and implementation of all Union policies and activities” [5]. The key difference lies in the later legal act referring to the right to healthcare, while the earlier one contemplated the right to health; however, both provisions suggest the state’s responsibility for ensuring the right conditions to allow citizens to enjoy and protect their health.
Inclusion of the right to healthcare in the Covenant on Economic, Social, and Cultural Rights corresponds to its association with the concept of positive freedom to have the individual’s needs and aspirations satisfied, which makes this right somewhat controversial in more liberal systems, such as the United States [6]. In the European social welfare and social insurance systems, on the other hand, it is a major element.
The right to enjoy health is rooted in and strongly intertwined with other basic rights. It is perceived as key to the right to life and dignity on one hand, and a precondition to enjoy any other rights on the other [7]. Importantly, the quality of healthcare services has a significant impact on such issues as the right to privacy, integrity, protection from torture or degrading treatment, and in some cases even the freedom of thought and religion.
Right to healthcare – Polish provisions
The Polish legal framework also provides for the right to healthcare, guaranteed in art. 68 of the Constitution: “Everybody has a right to healthcare” [8]. The second item of the same paragraph states that: “Public authorities ensure equal access to health care services funded by public resources to all citizens, regardless of their economic situa-tion”. This wording is a compromise between the intent to guarantee second-generation rights on one hand, and awareness of the state’s limited resources on the other [9].
Provision of healthcare is regulated by the major Act on Public Health [10], which defines the main tasks of the state in this area, the main actors involved, as well as the terms of funding. Therefore, this is the legal act that sets the framework of Poland’s health system, defined by the World Health Organization as the “ensemble of all public and private organizations, institutions, and resources mandated to improve, maintain, or restore health” [11]. The Polish act is supplemented by a range of specialist regulations concerning specific areas of healthcare (e.g. mental health), prevention (e.g. promotion of healthy lifestyle), medical education, etc. The Polish system is predominantly state funded, based on solidarity and striving to ensure universal healthcare, and thus corresponding to the Beveridge model [12]. Important regulations are also included in the specialist Act on Patients’ Rights and Patient Ombudsmen [13]. Apart from the fundamental right to healthcare services, the act contemplates patients’ right to information, confidentiality, informed consent, privacy, etc.
The COVID-19 pandemic necessitated broader introduction of telemedicine in Poland and other parts of the world. The respective legal provisions were introduced in August 2020 with the Regulation of the Minister of Health concerning organizational standards of tele-counselling within basic healthcare [14]. However, teleradiology had also been applied and regulated in Poland before the pandemic.
Increasing role of imaging in diagnostics and management
In contemporary medicine more and more objective data are necessary to make a precise diagnosis, to establish a proper treatment, and to follow up the results of the treatment. Imaging methods, especially CT and MRI, are among the crucial tools to provide the information mentioned above, and new imaging techniques like CT angiography, CT perfusion, MR perfusion, MR diffusion enlarge the diagnostic possibilities of imaging methods.
In most diseases, the use of imaging results is necessary to establish a diagnosis. Moreover, a report of an imaging study should include not only the suspected disease, but also more detailed information about the extent of the pathological process, which can be helpful to establish the treatment. For example, in patients with lung cancer a report of chest CT should include information on the size and location of the tumour, infiltration of the adjacent tissues, presence or absence of metastases to lymph nodes, lungs, bones, etc. This information is necessary for the referring physician to choose optimal management, e.g. surgical excision versus chemotherapy or radiothe-rapy.
The spectrum of diseases that require imaging information is constantly increasing. Emergency medicine is one of the fields in which this process is observed. Nowadays, most patients in emergency departments need to be referred to plain X-ray, sonography, or CT examinations. Cardiovascular imaging is another example. Due to technological developments, CT angiography has become the method of choice in diagnosing symptomatic stenoses or occlusions of vessels in all locations in the body.
Also, an increasing number of follow-up imaging studies are needed. In many diseases, it is necessary to perform imaging to evaluate the extent of the disease or the effect of the treatment. This is particularly important in oncology. Fortunately, with improving results of oncological treatment, patients with cancer can survive for many years, which means an increasing number of examinations as they undergo an imaging follow-up every few months, usually including CT or MRI of several body regions.
Finally, the guidelines of the national consultants, scien-tific societies, as well as the requirements of the National Health Fund have introduced mandatory performance of imaging studies in the therapeutic process. An example is MR in patients with prostate cancer, who, in the last decade, have become mandatory for staging prostate cancer with PI-RADS classification [15].
All the factors described above contribute to an increased number of imaging studies and their growing importance in the management of patients. This means that prompt performing and reporting of the imaging examinations contributes markedly to the final results of the therapeutic process. Therefore, there is a strong need to increase access to imaging, which requires an increase in both the number of imaging equipment and the number of radiographers and radiologists.
Deficiencies in the Polish healthcare system and radiology
In general, the Polish healthcare system is not efficient, burdened with multiple problems of a financial, organizational, and legal nature, and viewed by the society as one of the state’s leading problems [16]. According to Eurostat data for 2019 [17], Poland’s healthcare spending was not only lower than the average for the European Union member states, but its 6.5% of GDP was the third lowest rate in the entire European Economic Area. In absolute numbers, Poland’s expenditure of 902€ per inhabitant was also among the lowest results.
According to a report by the Supreme Audit Office of 2018 [18], the main issues in the Polish healthcare system start with funding, which translate into insufficient supply of healthcare services. The Audit Office highlighted deficiencies in educational and prophylactic services, resulting in unfavourable statistics concerning early detection of disease. Consequently, the healthcare system spent too much on intervention instead of prevention. In this context, access to diagnostic imaging studies was mentioned as second on the list of healthcare services with the highest waiting times for stable patients: 171 days of waiting in the case of MRI and 59 for computed tomography. The situation was worse only in the case of specialist out-patient care in endocrinology osteoporosis treatment, with average waiting time of 363 days [18].
In later years, the system was additionally burdened by the COVID-19 pandemic. It was not properly prepared for such a situation, which resulted in multiple shortcomings in providing healthcare to Polish citizens. In its 2021 report [19], the Supreme Audit Office concluded that “The audited hospitals providing healthcare services within the public system, were unprepared to operate in the circumstances of the COVID-19 pandemic, and changes in their organization failed to ensure the right functioning, and especially they failed to ensure the right access to health care services for patients other than those infected with SARS-CoV-2; and complete elimination of the risk of the pathogen’s spread among patients and medical staff”. Similar findings were reported by the Commission for Human Rights, whose report stated that the pandemic-related organizational changes in the healthcare system were “associated with lack of guidelines and uniform direction in activities […] leading to organizational chaos and disinformation among the medical staff, as well as patients” [19]. Thus, it can be concluded that the pandemic contributed to further deterioration of the functioning of the Polish healthcare system.
Funding
Accessibility of particular tests is significantly affected by funding possibilities. In the Polish healthcare system, public (through the National Health Fund – NFZ) and private (through one-to-one settlements at private practices or subscription schemes) funding co-exist. The costs of imaging studies performed at hospitals (including emergency departments) are covered by the hospitals’ budgets as the part of the diagnostic-therapeutic procedures paid by the National Health Fund. For example, the procedure for appendicitis treatment includes sonography and/or CT of the abdomen [20]. On the other hand, outpatient CT and MR studies are reimbursed directly by the National Health Fund, provided that patients are referred by specialists employed at institutions that have signed an agreement with the National Health Fund. Importantly, in the case CT and MRI, the public payer does not set limits to the number of studies according to Ordinance No. 37/2019/DSOZ of 29 March 2019 of the President of NFZ, and therefore the Fund pays for an unlimited number of imaging tests performed by healthcare institutions that have concluded the respective contract [21]. Thus, reimbursement of the outpatient CT and MR studies is unlimited, which means that any number of performed CT and MR examinations are paid for by the National Health Fund. Besides, there is a special unlimited path for imaging studies in oncological patients, and since November 2022 first-line general practitioners have been allowed to refer patients to chest CT.
The regulations mentioned above resulted in a rapid increase in the number of public and private CT and MR units that signed agreements with National Health Fund to perform an unlimited number of CT and/or MR studies with unlimited reimbursement. Therefore, funding of imaging studies is not a problematic issue. Instead, due to the rapid increase of imaging studies, the availability and quality of radiological equipment and the availability of medical staff have emerged as the main problems.
Equipment
According to Eurostat data [22], Poland recorded a significant increase in the ratio of both CT and MRI scanners per 100,000 inhabitants between 2010 and 2020. However, while in the case of CT units it ranked in the middle (15th spot out of the 27 EU member-states, on a similar level as Estonia, Ireland, and Spain), the ratio of MRI units in Poland was the fourth lowest in the EU (higher only than in Portugal, Slovakia, and Hungary). The data concerning the number of examinations are also worrying for Polish patients: Poland was characterized by the fourth lowest ratio of MRI examinations per 100,000 patients, followed only by Romania, Bulgaria, and Cyprus, and the ratio for CT examinations placed Poland as the sixth last member-state before Italy, Slovenia, Bulgaria, Finland, and Romania. The Eurostat data show clearly that while the number of units is an important parameter, the effectiveness of using their capacities differs in individual countries.
Detailed data concerning equipment owned by hospitals and its application are stored and disclosed by the Ministry of Health [23]. These data are shown in Tables 1 and 2.
Table 1
Computed tomography units and examinations in voivodeships
[i] Source: Biuletyn Statystyczny Ministra Zdrowia [Statistical Bulletin of the Minister of Health]. Sprzęt medyczny tomograf komputerowy, rezonans magnetyczny, mammograf [Medical equipment computed tomography, magnetic resonance, mammography] [23].
Table 2
Magnetic resonance units and examinations in voivodeships
[i] Source: Biuletyn Statystyczny Ministra Zdrowia [Statistical Bulletin of the Minister of Health]. Sprzęt medyczny tomograf komputerowy, rezonans magnetyczny, mammograf [Medical equipment computed tomography, magnetic resonance, mammography] [23].
The data show clearly that distribution of the units in voivodeships is uneven, leading to unequal access to medical services for inhabitants of different regions. There is also a difference in the availability of healthcare between urban and rural areas, confirmed by research concerning general access to hospitals, pharmacies, and doctor appointment, as well as waiting times: “Based on the research results, it was found that in 7 regions, rural population has good or very good access to healthcare, while in 9 regions, the access was restricted to a lesser or larger degree; moreover, within the analysed 8 years, accessibility of healthcare system services in the countryside has not improved in general” [24].
On the other hand, it should be stressed that equipment purchases and funding are not always well designed and adapted to patients’ needs. A report published in 2012 by the Supreme Audit Chamber’s concerning equipment purchased with Regional Operational Programs (development programs for each voivodeship, co-financed by the European Union’s structural funds) concluded that before buying the devices, “organs of public administration, Minister of Health, and local governments failed to diligently analyze the health needs and factors that affect their change” [25].
Another problem concerns the quality of the radiological equipment. The European Society of Radiology (ESR) recommends replacement of the radiological equipment (including CT and MR units) that is more than 10 years old, and careful maintenance of the equipment that is between 6 and 10 years old [26]. Poland does not follow this guideline. In fact, because the funding of CT and MR studies does not include a contribution to the replacement of the equipment, many CT and MR units that are more than 10 years old are still used. This affects the quality of the images, which could be further worsened during transmission of data in teleradiology.
Medical staff
Staff shortages are among the most urgent problems of the Polish medical system. In 2019, the Supreme Audit Chamber [27] found that “The basic problem of the [healthcare] system concerns the insufficient number of qualified medical staff and their uneven distribution, while the existing system for education and professional training of the medical staff does not guarantee the right number of sufficiently educated specialists consistent with the changing health needs of society. […] Discrepancies in distribution of medical staff in individual specialization have significant impact on access to selected healthcare services in the country.”. This problem is observed also in radiology.
According to the data of the Polish Supreme Medical Chamber [28], as of 30 November 2022, in Poland there were 189,324 doctors (physicians and dentists), and 173,828 of them were actually practicing medicine or dentistry. Of the overall number, 4476 were specialists in radiology and diagnostic imaging, and 4153 of them were actually working with patients. Similar data were published by Statistics Poland [29], showing that in 2019 there were 125,300 physicians working with patients in Poland, and 3.5% (about 4385) of them specialized in radiology and diagnostic imaging.
In 2022, the Supreme Audit Office published data on the number of physicians who were qualified specialists in radiology or diagnostic imaging in particular voivodeships (Figure 1) [30]. The data should be interpreted cautiously because they reflect all specialists and not only those who work on CT or MR examinations; however, the numbers allow a general estimation of discrepancies between particular regions in such indicators as the number of inhabitants per specialist radiologist, the number of specialist radiologists per CT and MR device, as well as number of examinations per specialist radiologist (Table 3).
Figure 1
Number of radiology specialists per voivodeship
Source: Najwyższa Izba Kontroli. Zakup i wykorzystanie wysokospecjalistycznej aparatury medycznej w podmiotach leczniczych. KZD. 430.008.2021 [30]
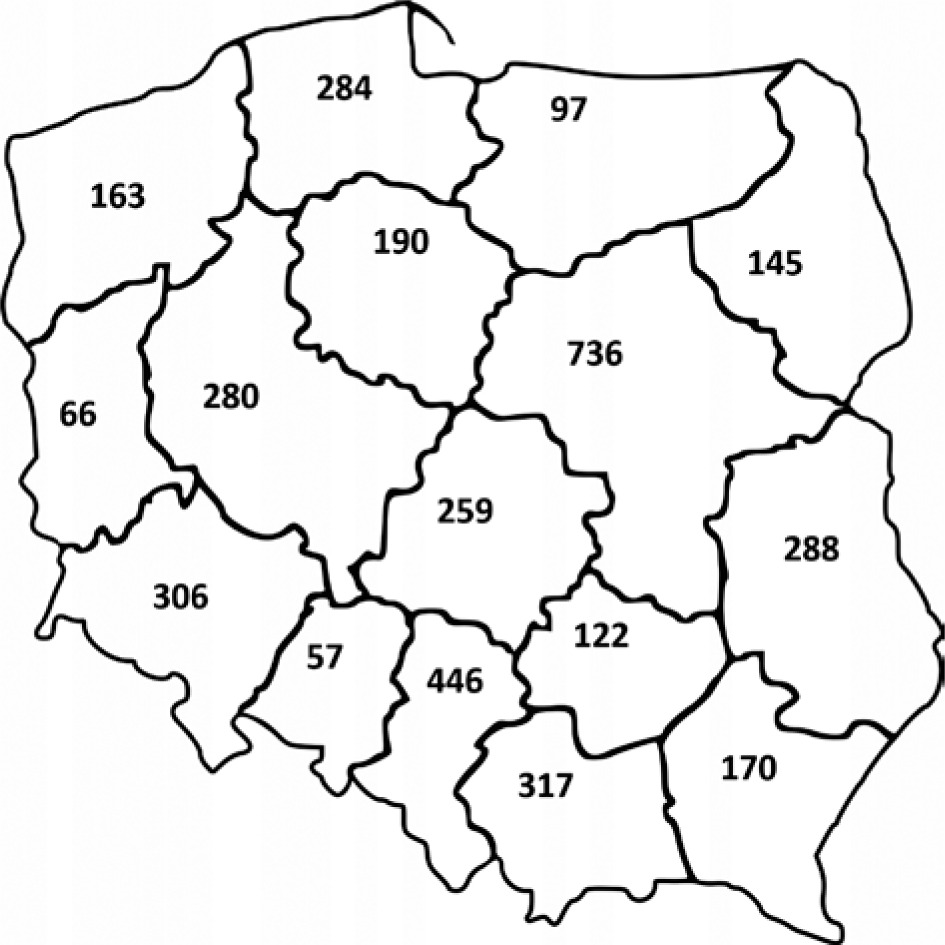
Table 3
Number of specialists in voivodeships
[i] Source: Najwyższa Izba Kontroli. Zakup i wykorzystanie wysokospecjalistycznej aparatury medycznej w podmiotach leczniczych. KZD. 430.008.2021. [30]
As in the case of the number of examinations per 10,000 inhabitants, there are clearly visible differences between voivodeships in terms of access to medical care related to availability of specialist radiologists. The number of patients per specialist differs largely, with the worst availability (Opolskie voivodeship) 2 and more than 2 times worse than in in the voivodeship with best availability (Lubelskie voivodeship). It is also important to note the potential staffing of the devices used in particular voivodeships, because the number of radiologists per device ranges from 2.85 to 6.45 in the case of CT units and from 5.94 to 13.33 for MRI units. The data show also that some voivodeships are better staffed with specialist radiologists, while others are clearly lacking.
An earlier report by the Supreme Medical Chamber [31] provides further details concerning the age of specialists and potential of replacement of current staff, as shown by the number of trainees in particular categories. It refers to demographic characteristics of the population of specia-lists in particular areas. With the share of physicians aged over 50 years at 53.0% in 2017, average age of 50.7 years, and median age of 50 years, radiology and diagnostic imaging ranked among the oldest groups of specialists. On the other hand, this specialization was one of those which recorded the highest increase of the number of specialists, e.g., between 2016 and 2017, the number of specialists radiologists grew by 130 physicians (seventh out of 78 specializations, behind internal medicine, cardio-logy, paedia-trics, orthopaedics with traumatology, family medicine, and anaesthesiology with intensive care), which translated into a slight decrease of mean age year-to-year (from 50.8 to 50.7 years old). This may be due to radiology and dia-gnostic medicine being relatively popular among young doctors, with 1106 young doctors pursuing the specialization residency program in this area in 2017.
Another factor that affects medical staff shortages is associated with the emigration of Polish doctors, which intensified after accession to the European Union in 2004 [32]. There is no information concerning the detailed data on specialization of the doctors who applied to the Medical Chamber for the respective certificate required to confirm their professional status abroad, but the overall numbers of several hundred doctors per year deciding to pursue their career abroad indicates a problematic tendency. It may have long-term consequences because such decisions are taken most frequently by younger physicians.
To summarize, the number of the radiologists in Poland is definitely insufficient, and the number of the newly trained specialists does not balance the increase in the overall number of the radiological studies (especially CT and MR), the decreased activity of the older generation of the radiologists (due to retirement or death), and emigration. Teleradiology could partially reduce this problem by improving the efficiency of the radiologists’ work.
Teleradiology potential
Development of IT systems causes a rapid increase in the number of radiologists who have access to teleradiology. Many public and private medical institutions are interested in providing technical facilities for teleradiology, or they sign contracts with teleradiology companies. The deve-lopment of teleradiology has increased the number of radiological reports, because radiologists can work at any time and any place all around the world, with just a good Internet connection and a computer. It is especially valuable in areas in which there are few radiologists. Therefore, teleradiology, along with increasing the number of trained radiologists and the development of artificial intelligence (AI) facilities, is considered as a most important way to overcome the problems of delayed radiological reports.
In 2020, while telemedicine was soaring in the COVID-19 pandemic, American scholars [33] identified 3 major fields of potential positive impact of teleradiology: “Technologic Progress and the Use of Artificial Intelligence”, “Teleradiology in Disaster Management, Humanitarian Efforts, and Mass Casualty”, and “Eliminating Disparities: Expanded Access to Imaging in Rural and Underserved Communities”.
Potential benefits may concern technological or orga-nizational matters. The application of centralized imageprocessing systems and establishment of massive databases of images and diagnoses may also assist in the development of AI tools to support analyses by radiologists. With respect to efficiency management, it improves crisis management by enabling the inclusion of human resources away from the disaster location. The highest and best adapted skills may be used without necessity to transport the radiologists.
In the Polish context, the possibility to manage medical staff shortages is especially relevant. While diverse sources of funding (state and local administration budgets, European Union funding, private sector, NGOs) allow the purchase of state-of-the-art devices by many medical institutions, and broad funding of healthcare imaging services promotes the availability of testing, the bottleneck involves access to highly qualified radiologists. Educating a physician is a long process, which only opens the path to specialization, and teleradiology may improve allocation, thus optimizing employment of the human resources available. In the context of migration of doctors, teleradiology may serve both to alleviate regional inequalities and to enable migrating doctors to cooperate with Polish healthcare units.
Teleradiology shortcomings
Teleradiology also has some shortcomings and risks. Hanna et al. [33] list among them the challenges of training and licensing of teleradiology specialists, the need for standardized regulations, technology issues, and financial settlement problems.
In the Polish context, one of the limitations concerns the cost of the required hardware and software (advanced computer, medical computer display, high-speed internet connection, etc.). However, most radiologists and medical institutions are able to cover these costs. Another associated problem involves the relatively high prices of services provided by teleradiology companies, which are increased by the profit of the company, overhead costs, etc. Therefore, many medical institutions agree to use the teleradiology services only of radiologists already employed at the institution, thus organizing hybrid work, partly on site and partly online.
The shortage of radiologists also affects teleradiology, because any radiological report, regardless of whether it is performed on site or online, consumes the time of the radiologist. However, radiologists who work entirely or partly in teleradiology can report more examinations because they save time for travel and administrative activities and can better organize the working time within a day or week.
Another disadvantage of teleradiology is worse supervision of the radiological examinations, because it limits the communication between the radiologist and radiographer. On the other hand, it should be mentioned that despite differences in setting and the lack of personal contact with the patient, radiographers, and other staff, a broad-scale German study [34] showed that the accuracy of teleradiologists is not significantly lower than in the case of on-site radiologists at on-call shifts.
Finally, the value of teleradiology is limited in emergency radiological examinations. Transferring images consumes time, which is crucial in emergency patients, e.g. with trauma or stroke. In these patients, treatment is often started based on the instant oral opinion of the radiologist. Therefore, in emergency conditions it is better to have an on-site radiologist or at least a radiology resident with the possibility of transferring the most important images to a specialist and having an online or phone consultation.
It should be stressed that most of these shortcomings are points requiring strict regulation and supervision rather than obstacles that cannot be overcome. Such regulations appear in legal provisions on one hand, and in best-practice guidelines on the other.
Legal regulations and health policy on teleradiology
In Poland, the term “teleradiology” is defined by the law in the Atomic Law Act [35] as “electronic transmission of radiologic images by transmission connection from one place to another for their assessment or consultation provided by a supplier who is independent from the healthcare unit where the image was created; the transmission does not cover internal-use transfer of images within a single healthcare unit”.
The basic terms of application of teleradiology are regulated by the specialized regulation of the Minister of Health concerning organizational standards of healthcare in radiology and diagnostic imaging provided via an information and communication system, initially introduced in 2019 [36]. Importantly, teleradiology can thus be applied for 2 different purposes: either a full, independent healthcare service replacing imaging reporting at the unit where the patient was imaged, or as a consultation service to confirm or verify the report.
The regulation contemplates 2 main points. One concerns ensuring the proper quality of the teleradiology report, firstly by a requirement that the service is provided by a qualified specialist (“holding 1st-grade specialization in X-ray diagnostics, radiology or radiodiagnostics or else 2nd-grade specialization or a specialist title in X-ray diagnostics, radiology, radiodiagnostics or radiology and diagnostic imaging – for radiographic studies; holding 2nd-grade specialization or a specialist title in X-ray diagnostics, radio-logy, radiodiagnostics or radiology and diagnostic imaging – for computed tomography, magnetic resonance or digital subtraction angiography”), secondly by ensuring the right transmission quality (“ensuring connection and electronic equipment allowing the relevant data transmission speed and quality (image and sound); ensuring that the physician […] has access to the radiographic image and a possibility to assess the correctness of the imaging while it is performed – for computed tomography, ensuring lossless compression of imaging data”), and thirdly, the right conditions of image assessment and reporting (“ensuring the right equipment and medical devices, including a reporting station, as well as conditions concerning reporting and reviewing radiographic images registered electronically”). Supervision of the quality of teleradiology services and fulfilment of the requirements are the responsibility of the institution that commissions teleradiology services.
The second point involves protection of teleradiology patients’ data, requiring “application of technical and organizational measures to ensure safe transmission of electronic documents in the graphic form (radiographic image) and in text (commission to perform a teleradiology service, price and radiographic image report) in manner guaranteeing their protection from unauthorized use”. This is in line with the binding principle of protecting patients’ rights, their privacy, and their personal data, as set both in the Polish [37] and international legal systems [38].
It should be highlighted that the provisions were introduced before the pandemic, and thus before the dramatic increase in the application of telemedicine in Poland. The teleradiology regulation is also more detailed in defining quality requirements than the later regulation on organizational standards in telecounselling in primary medical care [14]. However, teleradiology was not a major issue during the pandemic because limitation of direct patient-doctor contact is not among its major objectives.
Quality recommendations on teleradiology
Apart from binding legal requirements, there are also variable recommendations designed to ensure quality and consistence of teleradiology services throughout the given healthcare system. The most important are the guidelines developed by the specialist organizations of radiologists. Relevant provisions have been introduced in multiple countries, and below we will focus on documents issued by the European Society of Radiology – ESR [39], the American College of Radiology – ACR [40], and the Royal College of Radiologists – RCR [41].
The general frame for teleradiology at the European level was provided by the ESR in the “ESR white paper on teleradiology…” [39]. The main messages from this document are: “Teleradiology should form part of and be integrated with the wide spectrum of radiology services, and not a separate tradable commodity. The quality of radiological reports and services delivered by teleradiology should not be less than those of local radiologists. International quality standards for teleradiology need to be established. Patients need to be fully informed when teleradiology is used”. ESR’s White Paper refers to multiple elements that must be carefully considered to ensure this standard, including licensing of physicians working in teleradiology (quoting the European Diploma in Radiology and European Training Curriculum for Radiology as mechanisms to verify competencies), patients’ rights (e.g. the right to information that teleradiology services are applied, and informed consent), as well as technical issues. The document refers also to the necessity of providing effective bilateral communication between the referring and reporting physician, which also involves the need to tackle language issues.
The ACR’s document [40] similarly highlights such elements as patients’ rights, technical requirements, and continued quality improvement, proposing implementation of quality assurance systems including peer review or other mechanisms. The American document also analyses the working conditions of both on-site radiologists and teleradiologists, recommending that physicians in both groups have appropriate workstations, controlled working hours, and malpractice insurance. It further refers to economic and market conditions of supplying teleradiology services.
The 4 fundamental standards in the RCR’s document [41] provide for the relevant quality of data transfer, ensuring equivalent reporting standards by both on-site radiologists and teleradiologists, clear communication of results (including unequivocal marking of who prepared the report and contact between the referring and reporting physicians), and finally inclusion of teleradiology in the regular quality assurance systems as recommended by the RCR for all radiology services providers.
The basic points arising from the analyzed recommendations are summed up in Table 4.
Table 4
Guideline for high-quality and effective teleradiology
Conclusions
Teleradiology, like all telemedicine, is not a universal solution to all problems occurring in any healthcare system. It will not level unequal access to imaging, which depends on the region of the patient’s residence, as well as the difference between countryside and urban areas, especially big cities. However, it can help allocate available staff and competency resources better. Importantly, there have been legal provisions implemented in Poland, and there are quality guidelines available, including those by the European Society of Radiology, which also cover the Polish healthcare system. Therefore, there is a safe and constantly improved framework in place to monitor safety, quality, as well as economic viability of teleradiology solutions.
Consideration should be given both to the risks involved in teleradiology and those that arise from unequal access to medical care and problems with balancing needs and supply in emergency circumstances, such as natural disasters. Teleradiology should not be treated as an addition to fill in the gaps in the regular healthcare system; it should considered as a part of the system to ensure its better operation and management. Further efforts need to be taken to establish an optimal relationship between conventional on-site reporting of imaging studies and teleradiology, matched to the local personal and technical conditions. Communication tools and peer cooperation mechanisms should be in place to guarantee that both the referring and reporting physicians are able to perform the highest-quality work in the best interest of the patient and society in general.