Introduction
Ileocecal portion of the digestive tract bears the major brunt of many inflammatory and infectious diseases that affect the gut [1]. Ileocolonoscopy is a crucial investigation to detect the mucosal pathologies affecting the ileocecal junction of the bowel. Endoscopy may help clinch the diagnosis or narrow the differential diagnosis when typical mucosal lesions are seen [2,3]. However, in many cases the mucosal lesions of ileocecal region are atypical, rendering themselves to diagnostic dilemma [4-6]. Such mucosal lesions of uncertain diagnosis, especially in symptomatic patients, require careful evaluation to arrive at an appropriate diagnosis.
Ileocecal tuberculosis (ITB) and Crohn’s disease (CD) are 2 major disorders that affect the ileocecal junction. Ileocolonoscopy can clinch the diagnosis of CD or ITB in most patients when typical mucosal lesions are found [4], but in many instances, especially in early stages, both CD and ITB can present with non-specific or indeterminate mucosal lesions of the ileocecal junction on endoscopy [5]. Early ITB and CD usually have an overlapping clinical presentation. Thus, clinical symptomology and endoscopy cannot reliably differentiate between the 2 entities in many cases. However, it is essential to distinguish these 2 entities with certainty because the treatment for these 2 conditions is completely different, and the fallout of a misdiagnosis can have serious consequences [1].
Traditionally, barium studies were used to evaluate bowel lesions; however, they had limited sensitivity in the detection of early mucosal lesions and failed to demonstrate extraluminal findings. Nowadays, computed tomography enterography (CT enterography) using neutral oral contrast media has superseded barium studies for patients with suspected small bowel diseases [7-9]. CT enterography provides good luminal distention of the bowel, which helps in disease localization and assessment of various patterns of bowel wall involvement, and it demonstrates the extraintestinal findings. These findings can aid in making a definite diagnosis [10-12].
The present study was aimed to study the role of CT enterography in the evaluation of symptomatic patients who demonstrated ileocecal mucosal lesions of uncertain diagnosis on ileocolonoscopy.
Material and methods
Study design and patient cohort
This was a prospective observational study conducted in a tertiary care hospital, spanning a period of 2.5 years from July 2020 to December 2022. The study was approved by the Institutional Ethical Committee (IEC). Written informed consent was obtained from all the patients prior to the procedure.
All consecutive symptomatic patients aged more than 18 years who presented with new onset lower gastrointestinal symptoms (altered bowel habits, blood with stools, unexplained abdominal pain, mucus with stools, etc.) were subjected to ileocolonoscopy. Among these patients, those who had ileocecal mucosal lesions of uncertain diagnosis were enrolled in the final cohort. Ileocecal lesions of uncertain diagnosis on ileocolonoscopy were defined as mucosal inflammation, erythema, erosion, superficial ulceration, or nodules that did not fit into any particular diagnosis. Patients who had a history of prior intestinal resection or history of prior ATT or immunomodulatory (anti-TNF) treatment intake were excluded. We also excluded patients with stage 4 or 5 chronic kidney disease (glomerular filtration rate ≤ 30 ml/min) or those with any contraindication to CT scan like pregnancy or allergy to iodinated contrast media.
Patient preparation
CT enterography was performed within 10 days of ileocolonoscopy. All patients were prepared with a 24-hour residue-free liquid diet and complete fasting 4 hours before the study. Mannitol was used for distention of the bowel. 300 ml of 20% mannitol was mixed with 1 litre of water to form a total of 1.3 litres of the solution. The solution was administered orally over one hour (450 ml at 60 minutes, 450 ml at 50 minutes, 200 ml at 20 minutes, and 200 ml at 10 minutes before scanning). Sixty minutes prior to CT enterography 10 mg of oral metoclopramide was given in order to increase gastric and small bowel peristalsis, and 10 mg of hyoscine-N butyl bromide was administered to the patient just before scanning.
CT enterography protocol
All the CT enterography scans were performed with a 256-slice helical CT scanner (SIEMENS SOMATOM DEFINITION FLASH). A single breath-hold scan was obtained from the diaphragm to the symphysis pubis at a tube voltage of 120 kV, tube current of 30 mAs, and pitch of 0.6. The scans were acquired at a section thickness of 2 to 2.5 mm and reconstruction interval of 1.0 to 1.5 mm. Both non-enhanced and contrast-enhanced scans were performed. Non-ionic iodinated contrast material, iopromide (Ultravist, 300 mg/ml) was injected intravenously at a dose of 1.5 ml/kg of body weight and injected at a rate of 2.5 ml per second. Images were obtained approximately 45 seconds after the initiation of contrast material injection.
Image analysis
Two experienced abdominal radiologists (with 20 and 8 years of experience in abdominal imaging, respectively), who were blinded to the clinical and endoscopic details, interpreted the CT images. The 2 radiologists arrived at a diagnosis consensually.
The various intestinal and extra-intestinal findings on CT were assessed. The bowel was assessed for the location of the affected segment, location within the wall, mural enhancement, mural stratification, length of involvement, degree of thickening, type of thickening, submucosal fat deposition, pseudosacculation, ileocaecal junction involvement, mesenteric vascular prominence (Comb sign), mesenteric fat stranding, mesenteric fibrofatty proliferation, presence of stricture, fistula, lymphadenopathy, and ascites.
The findings were noted, and a diagnosis of CD and ITB was made on CT using the established imaging features already described in the literature [13,14]. A diagnosis of CD was made when typical imaging findings like symmetrical bowel wall thickening, mucosal hyper enhancement with stratified bowel wall appearance, discontinuous bowel wall involvement, terminal ileum predominance, comb sign, and small enhancing mesenteric nodes were detected. Similarly, a diagnosis of ITB was made when there was asymmetric bowel wall thickening, homogenous bowel wall enhancement with absence of stratified bowel appearance, ileocaecal junction/caecal predominance, large mesenteric lymph nodes with necrosis, and ascites were detected.
Patients in whom the CT enterography features were mixed with no clear pattern (some features resembling CD and others resembling ITB) were labelled as indeterminate.
The diagnosis obtained by CT enterography was correlated with the final diagnosis obtained from pathological data. Using descriptive statistics, the diagnostic performance of CT enterography was evaluated.
Results
A total of 178 cases were included, of which 25 cases were lost to follow-up during the course of the study. A total of 153 cases were finally enrolled in the study.
Clinical features and demographics
The demographic characteristics of the patients are presented in Table 1. Symptoms of abdominal pain and altered bowel habits were found to be commoner. However, no symptom was found to be specific for either CD or ITB (Table 1).
Table 1
Demographic parameters and clinical presentation of patients of Crohn’s disease (CD) and ileocaecal tuberculosis (ITB)
Ileocolonoscopy findings
On ileocolonoscopy, mucosal erosions/superficial ulcers were the commonest finding, present in 85.6% (131/153), followed by erythema in 81.7% (125/153) and nodularity in 21.5% (33/153). Other findings (like deformed IC junction and stricture) were present in 10.4% (16/153) of the cases.
Final diagnosis in patients undergoing CT Enterography
Among the total cohort of 153 patients, CT enterography findings suggesting ileocaecal pathology were present in 96% (147/153), and only 4% (6/153) of cases had a normal CT enterography impression.
On CT enterography a diagnosis of CD was made in 91 (59.5%) cases and ITB in 44 (28.7%) cases (Figure 1 and 2). A total of 12 (7.8%) cases were labelled indeterminate, and 6 (3.9%) cases were labelled as normal on CT enterography.
Figure 1
A 27-year-old male presented with history of fever and loose stools. Ileocolonoscopy showed erythema and ulcers of uncertain diagnosis in ileocecal region. Computed tomography enterography showed terminal ileal thickening with homogenous enhancement (arrow in A), multiple enlarged mesenteric nodes with some showing necrosis (arrow in B), and minimal pelvic ascites (arrow in C). Computed tomography enterography impression of ileocaecal tuberculosis (ITB) was given. Histopathology revealed caseating granulomas (D), confirming the diagnosis of ITB
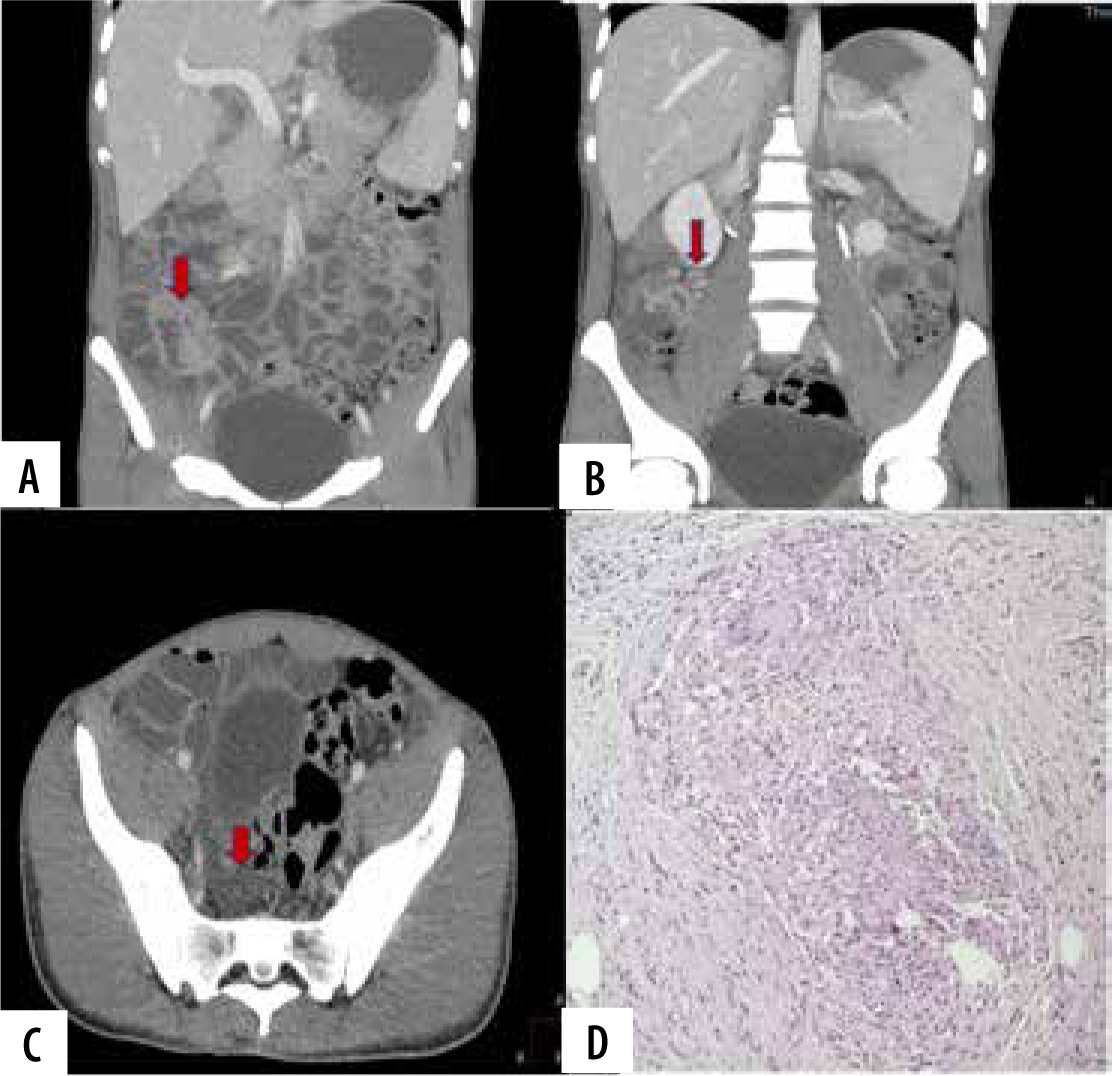
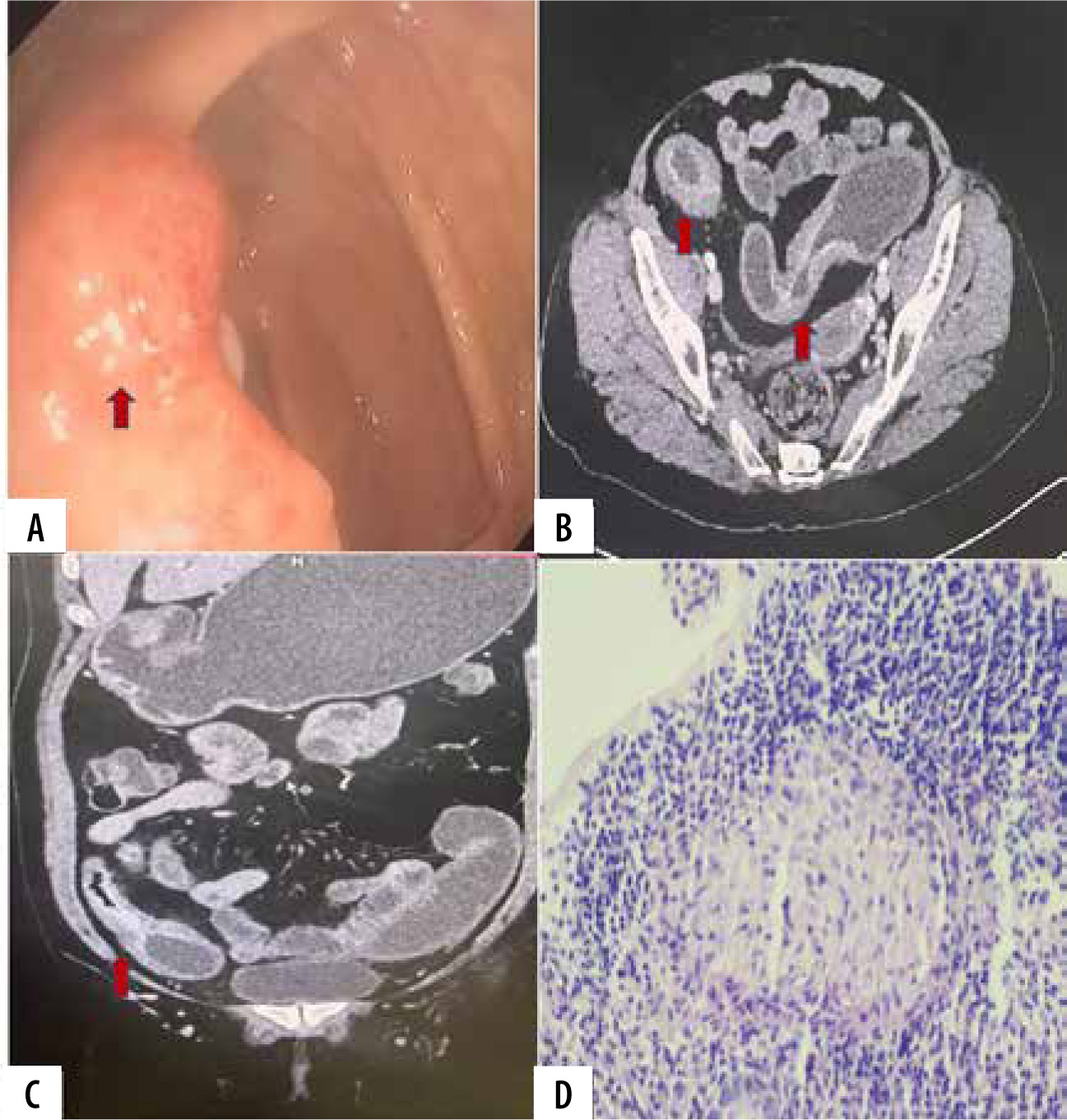
Figure 2
A 36-year-old female presented with 10-day history of pain in the abdomen and blood with stools. Ileocolonoscopy showed erosions and ulcers of uncertain diagnosis in the ileocecal region (arrows in A). Computed tomography enterography revealed bowel wall thickening with stratified mural enhancement in the terminal ileum (arrows in B and C) with mesenteric congestion (comb sign) and a few small enhancing mesenteric nodes. A CT impression of Crohn’s disease (CD) was made. Histopathology showed non-caseating granulomas (D) confirming the diagnosis of CD
Out of 91 cases who were given CT enterography impression of CD, a total of 76.9% (70/91) cases turned out to be CD on histopathological examination. Further 5.5% (5/91) of cases were confirmed as ITB, 8.8% (8/91) of cases were confirmed as infectious ileitis, and another 8.8% (8/91) of cases were indeterminate on histopathological examination.
Out of 44 cases who were given an CT enterography impression of ITB, 68.18% (30/44) of cases turned out be ITB on histopathology, whereas 18.18% (8/44) of cases were confirmed as CD, 4.5% (2/44) of cases were confirmed as infectious ileitis, and 9% (4/44) of cases were indeterminate on histopathological examination.
Out of the total of 12 cases who were given indeterminate CT enterography impression, 58.33% (7/12) turned out to be CD, 25% (3/12) of cases were diagnosed as ITB, and 16.66% (2/12) of cases were indeterminate on histopathological examination.
A total of 6 cases were given an unremarkable impression on CT enterography, out of which 66.7% (4/6) of cases turned out to be CD and 33.3% (2/6) of cases were confirmed as ITB on histopathological examination (Table 2).
Table 2
Computed tomography enterography and final diagnosis of the cases
CT enterography had a sensitivity of 78.65%, specifi-city of 67.19%, positive predictive value of 76.92%, negative predictive value of 69.35%, and diagnostic accuracy of 73.86% for diagnosing CD. CT enterography had a sensitivity of 75%, specificity of 87.61%, positive predictive value of 68.18%, negative predictive value of 90.83%, and diagnostic accuracy of 84.31% for diagnosing ITB (Table 3).
Table 3
Diagnostic performance of CT enterography for diagnosing Crohn’s disease (CD) and ileocecal tuberculosis (ITB)
Comparison of CT enterography findings between CD and ITB
A statistically significant difference was found between the type of thickening, type of enhancement, presence of ascites, presence of combs sign, presence of skip lesions, and presence of necrotic nodes between CD and ITB (all p-values <0.05) (Table 4).
Table 4
Comparison of computed tomography enterography findings between Crohn’s disease (CD) and ileocecal tuberculosis (ITB)
Diagnostic performance of various CT enterography findings in the diagnosis of CD
The diagnostic performance of different CT enterography findings in the diagnosis of CD is presented in Table 5. Symmetrical wall thickening and stratified mural enhancement had the highest sensitivity, specificity, PPV, NPV, and diagnostic accuracy, with all the statistical values exceeding 90%.
Table 5
Diagnostic performance of various computed tomography enterography findings in the diagnosis of Crohn’s disease (CD)
Diagnostic performance of various CT enterography findings in the diagnosis of ITB
The diagnostic performance of different CT enterography findings in the diagnosis of ITB is presented in Table 6. Necrotic mesenteric lymph nodes and asymmetrical bowel wall thickening had specificity of 99% and 96%, respectively, in the diagnosis of ITB.
Table 6
Diagnostic performance of various computed tomography enterography findings in the diagnosis of ileocecal tuberculosis (ITB)
CT enterography findings in non-specific infectious ileitis
Ten cases were confirmed as non-specific infectious ileitis. Mild bowel wall thickening was seen in 5 cases, moderate in 4 cases, and marked in one case. All the 10 cases exhibited symmetric bowel wall thickening. Mural stratification was maintained in all the cases of infectious enteritis. Segmental involvement was seen in 4 cases, whereas 6 cases exhibited diffuse involvement. One case had necrotic nodes.
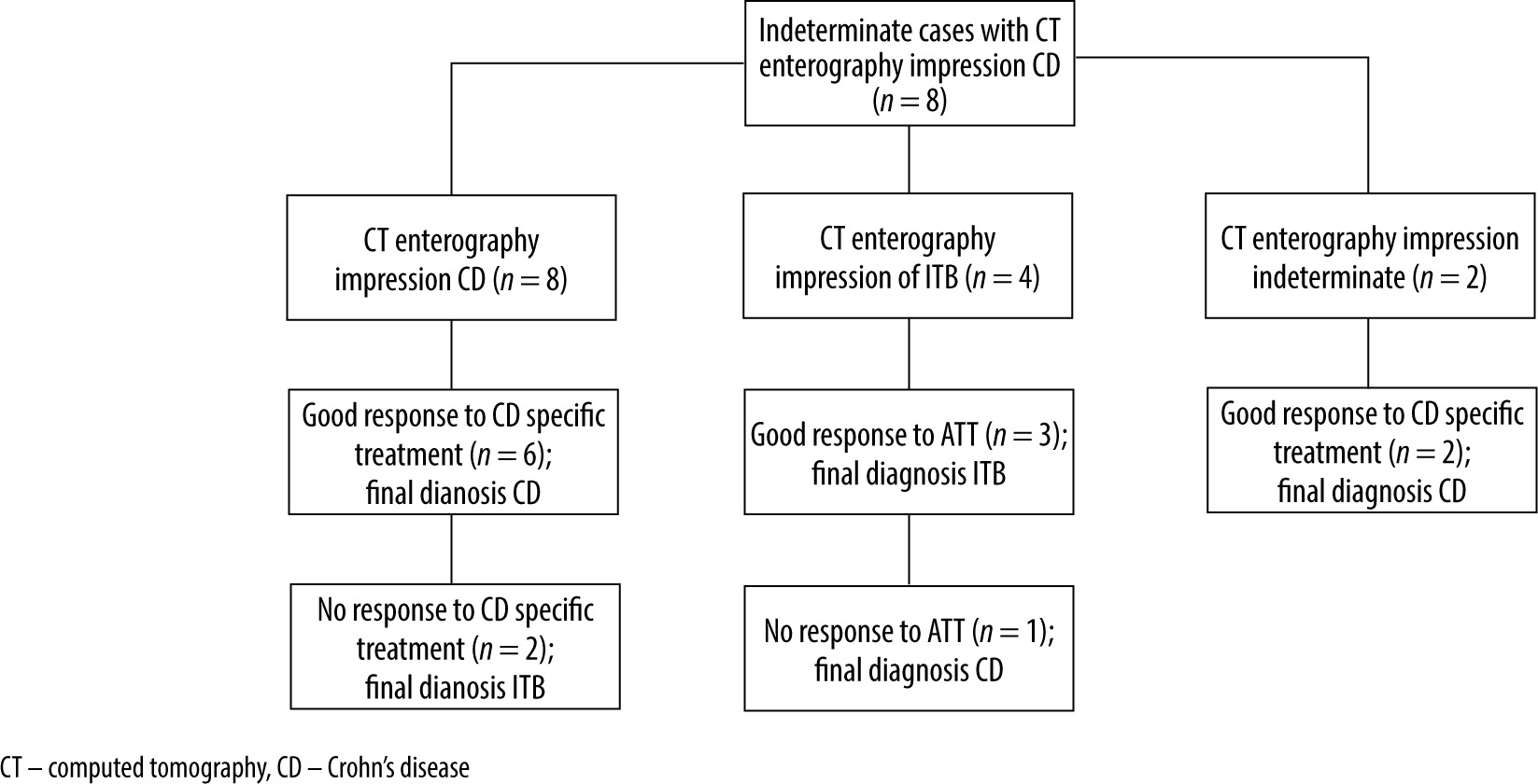
Indeterminate cases on histopathology
A total of 14 cases were inconclusive on histopathology. In such cases, CT enterography impression was used to guide empirical therapy. The outcome of these 14 cases is given in a flowchart (Figure 3). Based on response to empirical CD specific or anti-tubercular therapy, 9 out of these 14 cases proved to be CD, whereas the rest 5 were confirmed as ITB.
Discussion
CD and ITB comprise the bulk of diseases that affect the ileocaecal region of the gut with a minor contribution from other infectious ileitis (amoebiasis, salmonella) and inflammatory systemic disorders that affect the gut, like Behcet’s disease [1]. Developing countries that are at the crossroads of epidemiological transition are witnessing a rise in CD, which were previously endemic for ITB. A converse trend is being observed in many countries where the burden of ITB is increasing owing to the HIV pandemic. A confident distinction between ITB and CD is challenging for clinicians due to the overlapping symptoms. Certain clinical features like hematochezia and perianal involvement are common in CD, whereas night sweats and fever are common in ITB. On endoscopy the presence of aphthous or longitudinal ulcers is common in CD, whereas the presence of transverse ulcers or patulous ileocaecal valve is frequent in ITB. However, some patients have a non-specific endoscopic picture that is ambiguous. There are subtle histological differences between CD and ITB, and in many cases a confident distinction between the 2 diseases is difficult. On histopathology the detection of large caseating granulomas favours ITB, whereas the detection of microgranulomas favours a diagnosis of CD. Detection of acid-fast bacillus (AFB) is an exclusive feature of ITB. Although caseating granulomas or detection of AFB positive bacilli is pathognomonic of ITB, in up to 30% of cases there is a poor yield of endoscopic sampling. CT enterography offers the advantage of non-invasively assessing the entire bowel and extra-intestinal abnormalities and aids in differentiating between CD and ITB. On imaging, long segment discontinuous gut involvement, mesenteric hypervascularity are common in CD, whereas contiguous bowel involvement and presence of necrotic mesenteric lymph nodes favours ITB [12-16].
This study evaluated the role of CT enterography in the evaluation of ileocecal mucosal lesions of uncertain diagnosis on ileocolonoscopy. This study demonstrated a high diagnostic yield of 96% for CT enterography in ileocolonoscopy documented mucosal lesions of uncertain diagnosis. In this study CD (58.16%; 89/153) constituted the largest group, followed by ITB (26.14%; 40/153). A small percentage was confirmed as infectious ileitis (6.5%; 10/153). However, this does not reflect the general trend of disease in our community, where ITB still outnumbers the CD. This trend was peculiar to this cohort of patients who had an indeterminate endoscopic picture. The clinical symptoms were overlapping, and no symptoms were found to be specific to either CD or ITB.
On CT enterography hyperenhancing symmetrical bowel wall thickening (94.3% vs. 12.5%), preserved mural stratification (93.2% vs. 2.5%), skip lesions (70.7% vs. 17.5%), and increased mesenteric vascularity (comb sign) (80% vs. 10%) were significantly more common in CD compared to ITB (all p-values <0.05). In contrast, asymmetrical bowel wall thickening (87.5% vs. 4.5%) with homogenous enhancement, lack of mural stratification, presence of ascites (62.5% vs. 4.5%), and necrotic mesenteric nodes (100% vs. 0%) were significantly more common in ITB compared to CD (all p-values <0.05). These findings are in concordance with the studies of Kedia et al. [11], Kalra N et al. [15], and Choi D et al. [16], who reported that thick bowel wall with mural stratification pattern of enhancement is more common in CD. However, Zhao XS et al. [12] did not find any significant difference in patterns of bowel wall enhancement between CD and ITB.
In this study, the sensitivity of CT enterography for detecting CD and ITB was 78.65% and 75% respectively. Ray D et al. [17] observed a sensitivity of 93.75% for CT enterography in diagnosing ITB. The sensitivity of CT enterography has been reported in excess of 85% for diagnosing CD [18-21].
A study from India reported that CT findings of long-segment bowel involvement (69% vs. 28%), discontinuous bowel involvement (63% vs. 42%), positive comb sign (44% vs. 20%), and left colon involvement were more commonly associated with CD as compared to ITB. In contrast, frequent involvement of ileocecal junction (70% vs. 43%), short segment involvement, and lymph node size more than 1 cm (20% vs. 2%) were more common in ITB. The authors developed a predictive model based on CT features. They obtained a specificity of 90% and positive predictive value of 80% in diagnosing ITB when 3 characteristic CT features of ileocecal junction involvement, large lymph node size, and long-segment bowel involvement were present [11].
A study from China reported that asymmetric bowel wall thickening, segmental bowel involvement, positive comb sign, and proliferation of mesenteric fat were significantly associated with CD [22]. Discontinuous small bowel involvement and positive comb sign were found to independently predict the likelihood of CD, and the addition of these CT findings to endoscopic results significantly improved the diagnostic accuracy [23].
Another study from China concluded that CT enterographic parameters aided the differentiation between ITB and CD. This study showed that a mathematical regression model combining 6 parameters of clinical, endoscopy and CT enterography had a high sensitivity (97.8%), specificity (96.8%), accuracy (97.6%,), positive predictive value (98.9%), and negative predictive value (93.7%) for differentiation between ITB and CD [24].
A meta-analysis including 612 patients (CD 417; ITB 192) across 6 different studies reported that enlarged necrotic mesenteric lymph nodes were exclusively seen in ITB and had the highest diagnostic accuracy for ITB [25]. The presence of skip lesions and comb sign had a very high diagnostic accuracy for CD, with a sensitivity of 82% and specificity of 81%. Similarly, involvement of left sided colon, asymmetric bowel thickening, and mesenteric fat proliferation were found to have a poor sensitivity (40%) but good specificity (90%). Preserved mural stratification was found to have a poor diagnostic accuracy, possibly due to transmural bowel involvement in both CD and ITB.
There are still many challenges in the management of ITB and CD in areas that are highly endemic for tuberculosis, e.g. Asia. Hence, management strategies are often modified according to these challenges [26].
Recently a study demonstrated that a machine learning tool, namely the XGBoost algorithm, comprising 9 variables, has a high AUC, sensitivity, specificity, precision, and Matthews correlation coefficient (MCC), yielding values of 0.891, 0.813, 0.969, 0.867, and 0.801, respectively. The proposed framework concluded that the effectiveness of distinguishing CD from ITB through interpretable machine learning can obtain a good efficacy but may need an explanation for some individual patients [27].
Multiparametric-based predictive models incorporating clinical, endoscopy findings, histology, and radiology to differentiate ITB from CD are gaining popularity but have yielded varied results so far. Additionally, there is a lack of validation studies for most of such models [28].
Conclusions
The present study demonstrates the value of CT enterography in symptomatic patients who present a non-specific mucosal disease of ileocaecal junction on ileocolonoscopy. CT enterography has a high diagnostic yield in this subset of patients and aids in differentiating between the 2 most important chronic disorders of CD and ITB that affect the ileocaecal region of the gut. Symmetrical bowel wall involvement, preserved mural stratification, skip lesions, and comb sign favour a diagnosis of CD, whereas asymmetrical bowel wall thickening, loss of mural stratification, presence of ascites, and necrotic lymphadenopathy are significantly associated with ITB.