Introduction
Anomalous aortic origin of a coronary artery (AAOCA) refers specifically to the congenital anomaly in which a coronary artery arises from the opposite aortic sinus of Valsalva. In the literature, this anomaly is also frequently termed ACAOS (anomalous coronary artery from the opposite sinus).
The clinical expression of AAOCA is heterogeneous. Many patients remain asymptomatic, whereas others may present with exertional chest pain, reduced exercise capacity, or demonstrable ischemia. The greatest concern arises from its association with sudden cardiac death (SCD), particularly in young, otherwise healthy athletes. In a landmark study of 6.3 million U.S. military recruits between 1977 and 2001, 126 non-traumatic deaths were reported, of which 64 were cardiac in nature and 21 were attributed to AAOCA [2].
High-risk features of AAOCA include interarterial course, acute angle of take-off, slit-like ostia, and long intramural segments. All of these can be diagnosed in coronary computed tomography angiography (CCTA). However, because of the high heterogeneity of cases and low prevalence, their prognostic significance remains unknown. According to the recommendations of the European Society of Cardiology on congenital heart defects, the choice of treatment should depend on high-risk features, presence of symptoms, and documented ischemia in the area. In patients under 35 years of age with right anomalous course of the left main coronary artery (LMCA), surgery could be considered independently of other factors. In most patients, clinical decisions are made on a case-by-case basis, because scientific data are scarce and consist mostly of case reports [3].
Advances in cardiovascular imaging have markedly improved detection of AAOCA. CCTA is now regarded as the reference standard for anatomic delineation, given its ability to define the ostial location, proximal course, and high-risk features. Echocardiography, invasive coronary angiography, and cardiac magnetic resonance imaging play complementary roles in selected cases, particularly when functional relevance must be established.
It should be emphasized, however, that AAOCA represents only one subset of congenital coronary anomalies linked to SCD. Other high-risk variants include anomalous origin of the left coronary artery from the pulmonary artery or, more rarely, the right coronary artery (RCA) from the pulmonary artery [4]. In addition, certain presentations such as myocardial bridging, a single coronary artery, or AAOCA with an interarterial course between the aorta and pulmonary trunk are often termed “malignant” anomalies because of their recognized association with SCD [5].
Transthoracic echocardiography remains an important screening tool, particularly in younger patients [6]. In this setting, indirect signs such as the retroaortic anomalous coronary (RAC) sign and the binary left ventricular echo brightness (BLEB) marker may suggest the presence of AAOCA [7,8]. Post-mortem autopsy remains the definitive method for diagnosis in fatal cases. In contemporary practice, however, CCTA has become the predominant modality in many centers owing to its availability, high spatial resolution, and ability to comprehensively assess coronary anatomy. Invasive coronary angiography continues to have a role, though its capacity to identify certain high-risk features, such as intramural segments, is limited.
The present study focused on CCTA performed at a single institution between 2015 and 2022, with the aim of determining the prevalence and anatomical spectrum of coronary anomalies in the adult population. Particular attention was paid to distinguishing “malignant” from “benign” variants and to evaluating potential differences in prevalence between men and women. Such data may contribute to a better understanding of the clinical significance of AAOCA and its role in predisposing individuals to SCD.
Methods
We retrospectively reviewed 16,680 consecutive computed tomography (CT) examinations – both dedicated cardiac CT and chest CT studies – performed between 2015 and 2022 in the Department of Cardiovascular Imaging at our institution. All examinations were acquired on a dual-source 128-slice CT scanner (SOMATOM Definition Flash, Siemens Healthineers, Forchheim, Germany). Indications for CT were consistent with contemporary guideline recommendations.
Inclusion criteria: Patient records were systematically screened using an automated search algorithm to identify reports containing a description of a coronary artery anomaly. Only cases with a documented coronary anomaly were included for analysis.
Exclusion criteria: Patients were excluded if (1) the original CT dataset was unavailable, (2) the anomaly description was incomplete or non-diagnostic, or (3) the patient was younger than 18 years at the time of imaging (Figure 1).
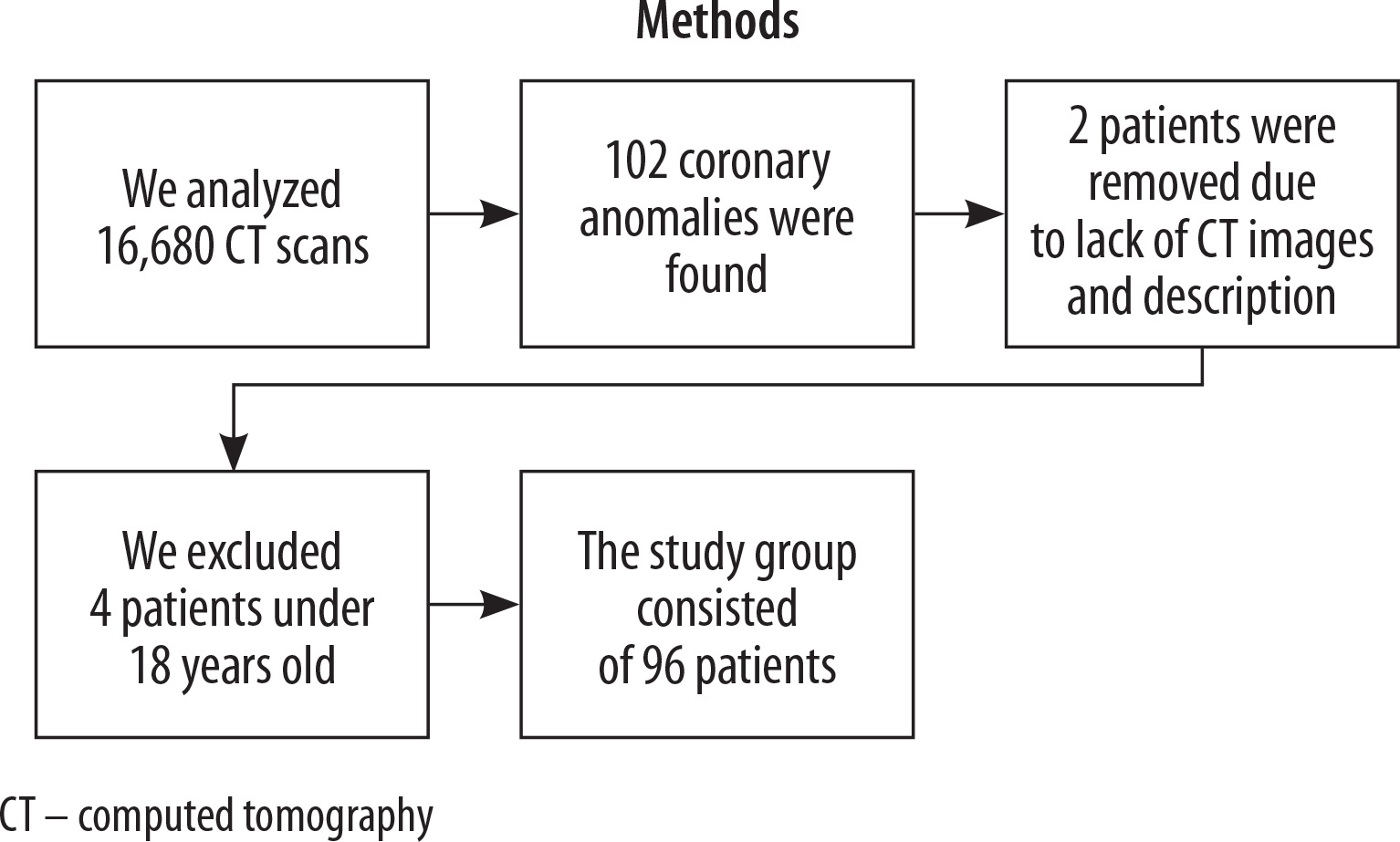
Automated text analysis of radiology reports from 16,680 CT examinations was performed to identify cases of AAOCA. A total of 102 cases were initially identified. Four studies were excluded because the patients were younger than 18 years. Two additional cases were excluded due to an incomplete radiological description and the absence of the corresponding CT dataset, which prevented verification of the anomaly.
Following exclusions, all eligible cases were entered into a dedicated registry. For each patient, demographic data (age and sex) and detailed information regarding the coronary anomaly were recorded. The data were subsequently organized and analyzed using Microsoft Excel (Microsoft Corporation, Redmond, WA, USA). Descriptive statistics were applied, and the results are presented in this report.
Results
Group characteristics
Patients enrolled in this study underwent no additional selection beyond that mentioned in the above section (Figure 1). They represented a cross-section of the study population during the specified time period. CT scanning was ordered for these patients for reasons consistent with current guidelines; it was not performed for non-medical reasons.
It was a single-center study from a clinic with the highest reference degree, gathering patients from the Polish population. The study analyzed a group of 96 patients. It consisted of 54 (56.25 %) men and 42 (43.75 %) women. The median age was 61 years (arithmetic mean age was 58.8 years).
Point of origin
According to the classification of Cheezum et al. [1], the following were included: RCA from left anterior sinus with anomalous course, LMCA from right anterior sinus with anomalous course, left anterior descending artery (LAD) from RCA, RCA from LMCA, LAD from right anterior sinus with anomalous course, and left circumflex artery (LCx) originating from the right side (R-LCx). Anomalous origin of the LCx from the right side has been described previously [9], but in our case this type of classification was not applicable. Therefore, we distinguished LCx originating from the RCA and LCx originating from the right coronary sinus, without further detailed classification into types. One more person with LCx originating from the right sinus was also found, who will be included among the patients with several overlapping anomalies. Due to the insufficient quality of the scans and for the sake of simplicity, LCx originating from the right coronary sinus from both the separate and common ostium will be included in one group.
The remaining anomalies of the artery outlet were single cases, which will be described individually later in the article.
The most common anomaly of the artery origin is the anomaly of the LCx origin from the right sinus of Valsalva. There were 48 such cases, which constitutes 50% of all anomalies found in the studies (Table 1).
Table 1
Types of anomalies and their courses
[i] L-RCA – left anomalous origin of right coronary artery, LCA – left coronary artery, n/a NCC-LMCA – non-coronary cusp origin of left main coronary artery, n/a – not applicable, NCC-RCA – non-coronary cusp origin of right coronary artery, R-LAD – right anomalous origin of left anterior descending artery, R-LCx – right anomalous origin of left circumflex artery, R-LMCA – right anomalous origin of left main coronary artery
The second most common origin anomaly is the RCA from the left anterior sinus with an anomalous course, found in 17 patients (left anomalous origin of right coronary artery, L-RCA). The third most common anomaly is the origin of the LAD from the right sinus, found in 12 patients.
In two patients, a coronary artery with an LMCA course was found arising from the RCA. There was also one case of a patient who did not have the LMCA, and an artery with a vascularization characteristic of the LAD arising from the RCA (right anomalous origin of left anterior descending artery, R-LAD). In their case, the LCx arose directly from the pulmonary trunk. Another anomaly involved a dual left coronary artery. One of the arteries branched off the LAD with a preaortic course. The LCx arose directly from the left coronary sinus. The next anomaly was the fusion of the left and right coronary cusps (LCC and RCC) and the departure of the RCA from the place where these cusps joined. However, this took place in the right coronary sinus. A similar case, but belonging to the RCA origin from an abnormal sinus, concerned the origin of the RCA from between the right and left coronary sinuses. Another patient was found to have a coronary artery anomaly consisting of the RCA originating from the anterior part of the aortic root. In another case, the RCA artery arose as a branch of the LAD. There was also a case where the RCA originated in the ascending aorta, in the left lateral wall. In the next patient, a complex anomaly was found, in which, in addition to the RCA, the LAD also branched from the right coronary sinus. A vessel with vascularization characteristic of the first diagonal branch and/or LCx originated directly from the aorta, precisely from the left anterior part of the aortic root. There was also a case of a patient with an anomaly consisting of origin of both the LAD and LCx from the right coronary sinus; additionally, the LAD had an interarterial course, and the LCx had a retroaortic course. The last case involved the origin of all coronary arteries from the right sinus of Valsalva.
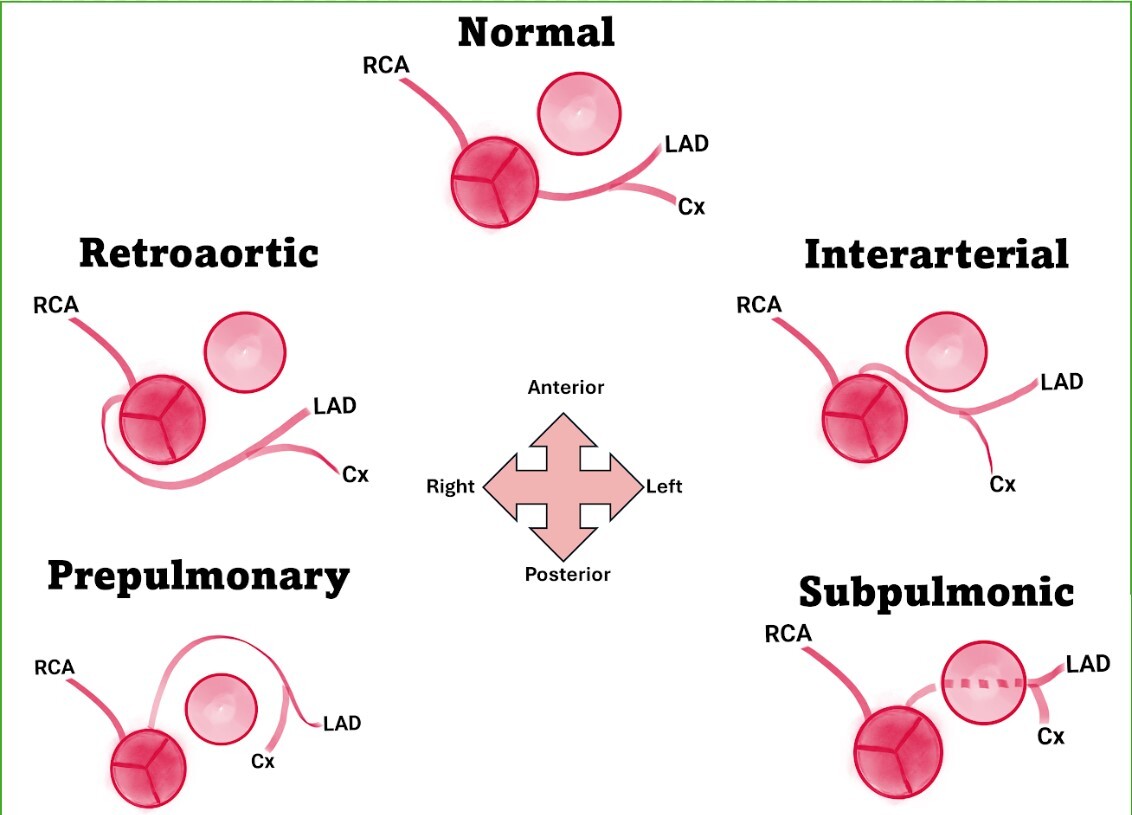
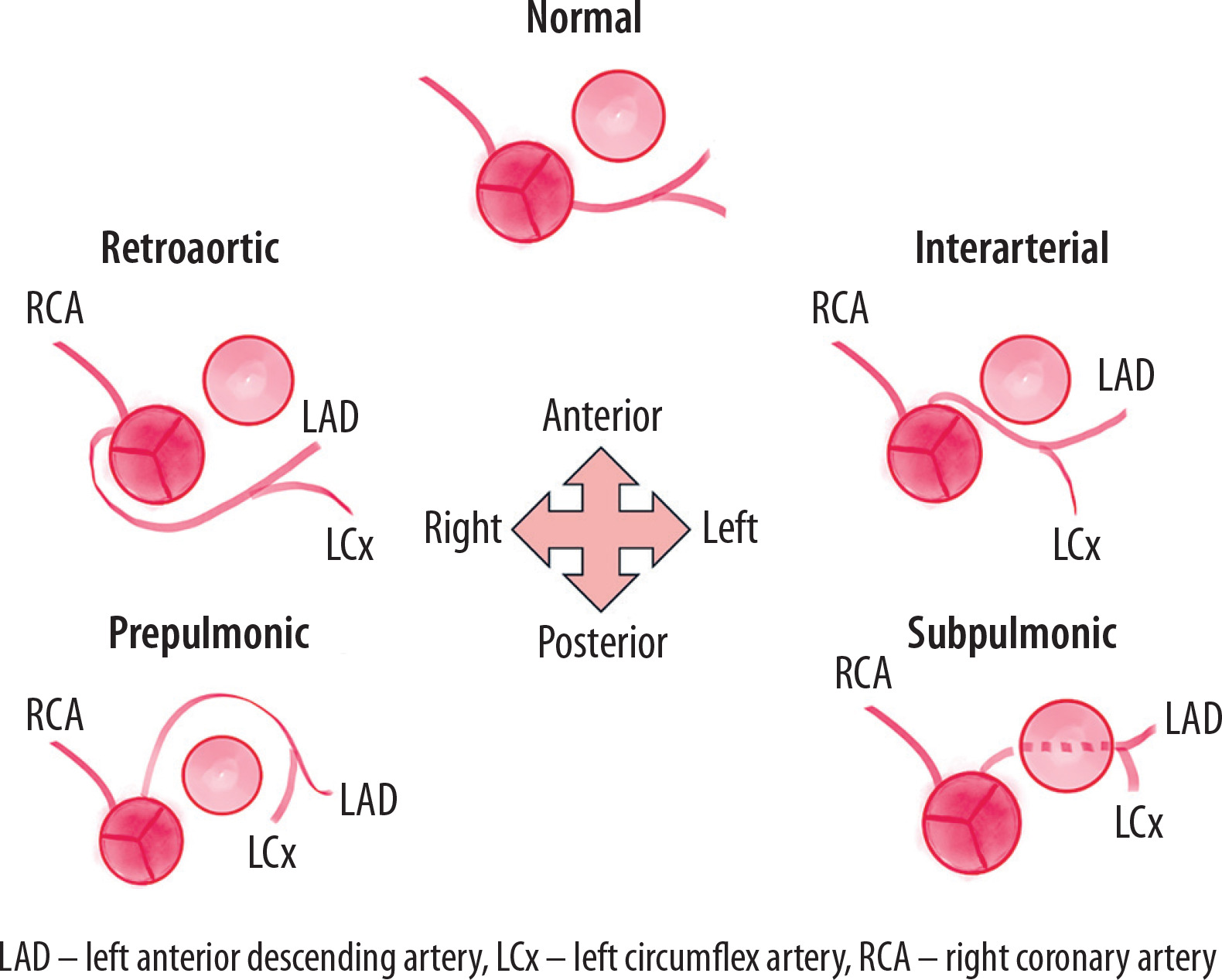
Course
Arterial course anomalies were classified in 82 of the 96 patients (Figure 1). In the vast majority of cases (47), a retroaortic course was identified. In 27 patients, the anomalous artery course was between great vessels, referred to as interarterial. The interarterial course is of particular importance because it is often associated with SCD [10], and it is also referred to as a ‘high risk’ course.
This is especially significant because this type of anomaly is particularly correlated with sudden death in young athletes [11]. Among patients diagnosed with AAOCA, two cases were identified with a retrocardiac course and two with a prepulmonic course. None of the patients in our group had a subpulmonic course. Additionally, in two patients, we found anomalies in more than one artery, so these individuals will be counted separately.
Remaining cases regarding course
In one patient, we found LAD from the right sinus with an interarterial course and LCx from the right sinus with a retroaortic course. The second patient had an interarterial LAD and a retroaortic LCx. This represents a rare anomaly in which all coronary arteries originate from the right coronary sinus (Figure 2).
Discussion
This study represents one of the largest single-center cohorts of patients with AAOCA analyzed using CCTA. This work, aggregating data from thousands of CT scans, revealed that AAOCAs were found in 0.58% of scans. In the general population, the condition is estimated to be present in 0.43-5.79% of patients [12]. The findings demonstrate that AAOCA is a relatively frequent observation in clinical practice. The LCx was the most common vessel involved, with the majority of cases exhibiting a benign course. Importantly, no malignant variant of R-LCx origin was identified in our cohort. These observations are consistent with the recognized variability of the LCx, which has the greatest freedom of trajectory among the epicardial coronaries.
Interpretation of AAOCA requires careful consideration of risk features. High-risk anatomical characteristics include an interarterial course between the aorta and pulmonary trunk, acute angle of take-off, slit-like ostium, and long intramural segments – all of which can be accurately visualized with CCTA. Nevertheless, their prognostic significance remains incompletely defined, largely due to the heterogeneity of presentations and the rarity of individual subtypes. Consequently, current evidence does not support uniform management guidelines. The 2020 European Society of Cardiology guidelines on congenital heart disease recommend that, in addition to high-risk imaging features, decision-making should take into account the presence of symptoms and documented ischemia in the territory of the anomalous artery. A notable exception applies to left coronary arteries arising from the right sinus, where in patients younger than 35 years, surgical correction may be considered irrespective of symptom status [9]. Beyond this, therapeutic decisions for AAOCA are most often individualized, reflecting the limited data available, with much of the literature confined to case reports or small series.
In our cohort, most patients were diagnosed by CCTA, which offers key advantages in assessing the three-dimensional course of anomalous vessels and in characterizing risk features. Although invasive coronary angiography remains widely used, its two-dimensional nature may hinder recognition of complex proximal courses, particularly in AAOCA. Transthoracic echocardiography also plays a growing role, especially in younger patients, where indirect signs such as RAC and BLEB can provide useful diagnostic clues.
The proportion of malignant courses is of central importance, given their association with SCD. In this study, interarterial courses accounted for 28.1% of cases, and were found predominantly in men (70.37%). Notably, the R-LCx anomalies did not demonstrate malignant features, whereas malignant courses were more commonly observed in L-RCA and R-LAD variants. These findings underscore the importance of systematic evaluation of coronary trajectory and vessel-specific risk.
The principal strength of this study lies in its large sample size from a high-volume imaging center, allowing reliable description of anatomical patterns. However, as a single-center retrospective analysis, the results may be influenced by referral bias, with enrichment for symptomatic or clinically suspected anomalies. Broader generalizability will require multicenter registries. In this regard, ongoing initiatives such as the EuroAAOCA registry represent an essential step toward establishing a comprehensive evidence base, enabling more accurate risk stratification and guiding management strategies for patients with AAOCA [13].
Comparison with other studies
The largest study describing AAOCA [14] evaluated 90,501 patients. The study had a similar methodology, i.e., retrospective assessment based on CT scan results. 207 AAOCAs were found, with a prevalence of 0.23%. The results of this study may not be an accurate reference point due to the different population, as it was conducted in China. Therefore, ethnic differences may limit its applicability in other populations. A similar study [15] conducted on a population-based cohort of 89,314 patients from five hospitals assessed the incidence of right-sided AAOCA from the left coronary sinus with an interarterial course. This course was found in 0.354% of patients. Another study conducted on a group of 390 patients with previously diagnosed AAOCA showed an LCx anomaly in 54.4% and an RCA anomaly in 31.3% of participants [16]. In a study aimed at assessing the incidence of AAOCA using echocardiography, the percentage of detected anomalies was 0.0078%. However, the difference in percentage is most likely due to the lower sensitivity of echocardiography in detecting AAOCA compared to CT [17].
Limitations
This study may be limited by the retrospective collection of the study group. Verification of anomalies in some cases may lead to underestimation of the occurrence of a specific type. It is also impossible to obtain the original CT scans, especially in studies performed long ago, necessitating reliance on radiological descriptions. This is often the case in this field, as the rarity of AAOCA makes it impossible to collect a sufficiently large group in a prospective study. Additional limitations may be related to the sensitivity of the diagnostic method itself, although the possibility of CT analysis in 3D reconstruction provides an advantage over the commonly used angiography.
Conclusions
It is important to note that the data from our study were derived from patients who were being diagnosed for other reasons than the suspicion of AAOCA, and few of them were completely asymptomatic. Thus, our data reveal the percentage of coronary anomalies in cardiac patients undergoing tomographic imaging, and may be relatively low due to the characteristics of the participants.
Incidental findings pose a clinical problem for healthcare professionals and their patients: coronary anomalies are associated with increased risk of ischemia, myocardial infarction and SCD. However, surgical procedures also pose a risk to the patient. Even pharmacological treatment, although considered to be safer, can cause complications. Decisions about exercise restriction and surgical procedures should be made after discussing risks and benefits of available methods with the patient. This is especially important in asymptomatic patients, who would not seek treatment if their condition was not revealed incidentally.