Introduction
Left ventricular hypertrophy (LVH), defined as an increase in left ventricular (LV) wall thickness or LV myocardial mass, is commonly encountered in clinical practice. LVH is induced by several mechanisms, including physiological adaptation to increased afterload, structural diseases, and excessive accumulation of metabolites [1,2]. Hypertrophic cardiomyopathy (HCM) and its phenotype refer to LV myocardial wall thickness ≥ 15 mm, or ≥ 13 mm in combination with family history of HCM in at least one myocardial segment [2]. The severity of LVH is closely associated with major cardiac events across various populations [3,4]. It is clinically important to estimate LVH accurately and determine the etiologies of LVH for appropriate treatment.
Cardiac magnetic resonance imaging (MRI) is useful for determining the etiologies of LVH and stratifying the risk of major cardiac events, owing to its wide range of view, reproducible assessment of cardiac morphology and function, and excellent tissue characterization compared to other imaging modalities [1,2,5,6]. Another advantage of MRI is that it does not require irradiation. Notably, the myocardial tissue alterations visualized by MRI are consistent with the pathological findings [7,8]. Therefore, cardiac MRI is also used to monitor changes in LVH, cardiac function, and myocardial tissues during and after the treatment for each etiology of LVH [9-13].
The etiologies of LVH are diverse; therefore, the clinical utility of cardiac MRI is maximized when combining with patient-specific information, including patient’s age and family history. For example, the onset of LVH in childhood and adolescence suggests hereditary or metabolic diseases as the etiologies of LVH and high risks for sudden cardiac death (SCD) [14-16].
In this review we describe the clinical information necessary for interpreting cardiac MRI in LVH. Appropriate MRI sequences for differentiating and monitoring LVH are described concisely. We guide the interpretation of cardiac MRI of LVH through clinical examples acquired in daily practice.
Clinical information necessary for interpreting cardiac MRI of LVH (Table 1)
Symptoms
Chest pain or dyspnea during daily activities is a common symptom of LVH that disrupts the balance between the blood supply and demand of the hypertrophied myocardium. In particular, this symptom is associated with massive LVH or stenosis of the LV outflow tract (LVOT) induced by hypertrophic obstructive cardiomyopathy (HOCM) or aortic stenosis [10,17]. Syncope is induced by arrhythmic events, significant changes in blood pressure, or a decrease in stroke volume [5,10,14,17]. Heart failure may be the initial symptom of hypertensive heart disease (HHD) and cardiac amyloidosis [18,19]. Heart failure predicts a worse prognosis in HCM, cardiac amyloidosis, and aortic stenosis [14,17]. Unfortunately, SCD is an initial symptom in some patients with HCM, who can be young athletes [14,20]. Indeed, approximately half of SCD in young athletes is attributed to HCM [20].
Table 1
Clinical information necessary for interpreting cardiac magnetic resonance imaging of left ventricular hypertrophy
Ages
The onset of LVH in children and adolescents indicates hereditary cardiomyopathies or congenital metabolic diseases as the etiologies of LVH [14-16]. These diseases include HCM, glycogen storage disease, and Noonan syndrome. SCD in young athletes is attributed to HCM [20]. HCM and Anderson-Fabry disease may develop in middle-aged and older individuals according to sex, gene penetrance, phenotypes, and environmental factors [10,21,22]. HHD, cardiac amyloidosis, and aortic stenosis are observed in older adults, except for aortic stenosis associated with a bicuspid aortic valve [11,17-19].
Sex
LVH is often found in men, because HHD and HCM are observed more frequently in men than in women [9,18,22]. By contrast, LVH and heart failure with preserved ejection fraction (HFpEF) induced by hypertension is observed in older women [23]. HCM, which is the most common primary cardiomyopathy, occurs more frequently in men than in women, irrespective of its autosomal dominant inheritance [22]. Conversely, HOCM refractory to pharmacological treatments is commonly investigated in older women [10,22]. More than 90% of wild-type transthyretin (ATTR) cardiac amyloidosis is observed in men [11].
Body mass and appearances
HHD is often associated with obesity, especially when LVH and HFpEF coexist [23]. Obesity is reported to induce adverse long-term outcomes in patients with HCM [24]. Characteristic appearances and growth retardation strongly indicate hereditary or congenital metabolic diseases, such as mitochondrial cardiomyopathy and Noonan syndrome [16,25].
Family history
A detailed review of family history is important because its presence is a strong clue for the hereditary etiology of LVH and is significantly related to the prognosis of patients with LVH [14,15,21,26]. Family history indicates the modes of inheritance of each etiology, such as autosomal dominant, recessive, or X-linked recessive. Genotypes are not directly related to the phenotypes and prognoses of LVH, whereas a family history of cardiomyopathies – which encompasses genotypes, genetic modifiers, environmental factors, and phenotypes – is significantly related to the prognosis of HCM [22,26].
Noncardiac past history
Some types of noncardiac past history indicate the etiology of LVH. A history of carpal tunnel syndrome and lumbar spinal canal stenosis indicates wild-type ATTR amyloidosis, while polyneuropathy suggests hereditary ATTR amyloidosis [19]. Neuropathic pain, dermatological manifestations, and hypohidrosis in childhood suggest Anderson-Fabry disease [21]. Cerebellar ataxia and hearing impairment are observed in mitochondrial myopathy [25]. Much attention should be given to “noncardiac” history in patients with LVH.
Cardiac MRI sequences for evaluating LVH (Table 2)
Cine steady-state free precession imaging
Cine steady-state free precession (SSFP) MRI has been established as the gold standard for measuring cardiac function owing to its high reproducibility. Because of the unrestricted view, cine SSFP can measure the basal anterior septal, high lateral and apical wall thickness accurately [16,27,28]. Another advantage of cine SSFP is its ability to measure the wall thickness and function of both the atria and right ventricle [27]. SSFP is sensitive to fluid collection, such as pericardial and pleural effusion, which is associated with cardiac amyloidosis.
Table 2
Relationship between cardiac magnetic resonance imaging sequences and etiologies of left ventricular hypertrophy (LVH)
[i] APH – apical hypertrophy, ASH – asymmetrical septal hypertrophy, CKD – chronic kidney disease, ECV – extracellular volume fraction, HCM – hypertrophic cardiomyopathy, HHD – hypertensive heart disease, LGE – late gadolinium enhancement, LV – left ventricular, MVO – midventricular obstruction, SSFP – steady-state free precession, T2 – T2-weighted imaging, ↑ – increase, ↓ – decrease, * – when organs are in field of view
T2-weighted imaging
The relationship between high intensity on the T2-weighted imaging (T2) and unexpected syncope is reported in asymmetrical septal HCM [29].
Parametric mapping
Parametric mapping provides quantitative parameters reflecting myocardial fibrosis, edema, and metabolites. The extracellular volume fraction (ECV) calculated from pre- and post-contrast T1-weighted imaging (T1) mapping quantifies the interstitial space in the myocardial tissues, and it is significantly related to the severity and prognosis of LVH [9,11,30]. In Anderson-Fabry disease, myocardial T1 is peculiarly shortened because of the accumulation of lipids [1,2,12,30]. Cardiac amyloidosis has a longer T1 and higher ECV than other etiologies of LVH [1,2,8,19,30]. T2 mapping can provide quantitative information about myocardial edema associated with LVH [12,27].
Late gadolinium enhancement imaging
Because late gadolinium enhancement (LGE) imaging visualizes myocardial fibrosis and scarring, which is a sequela of various types of myocardial damage, it is valuable for differentiating the etiologies of LVH [2,21,31,32]. Additionally, the presence, location, or extent of LGE is significantly related to the prognosis of patients with most etiologies presenting with LVH [2,14,33-36]. For example, HCM with LGE >15% of the LV myocardial mass shows a 6% risk of SCD at 5 years [33]. In HCM patients with extensive LGE, the installation of an implantable cardioverter defibrillator (ICD) can be recommended to prevent SCD [5,33]. LGE MRI has a pivotal role in cardiac MRI of LVH.
Cardiac MRI of etiologies presenting LVH (Table 2)
HHD
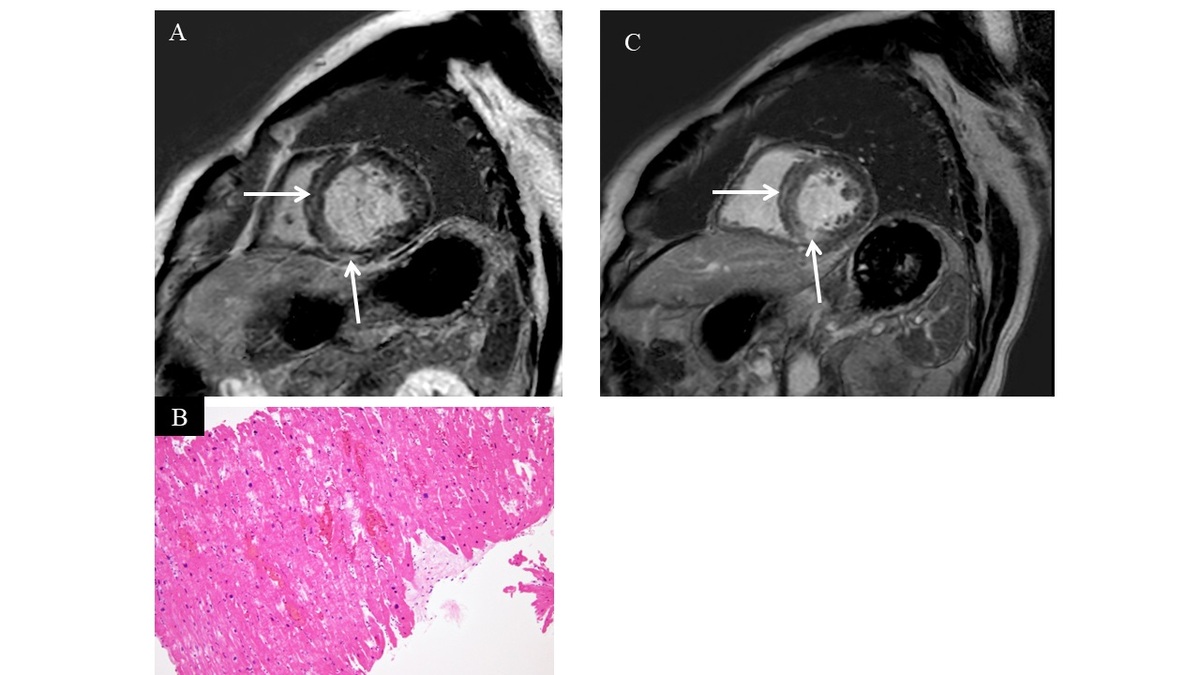
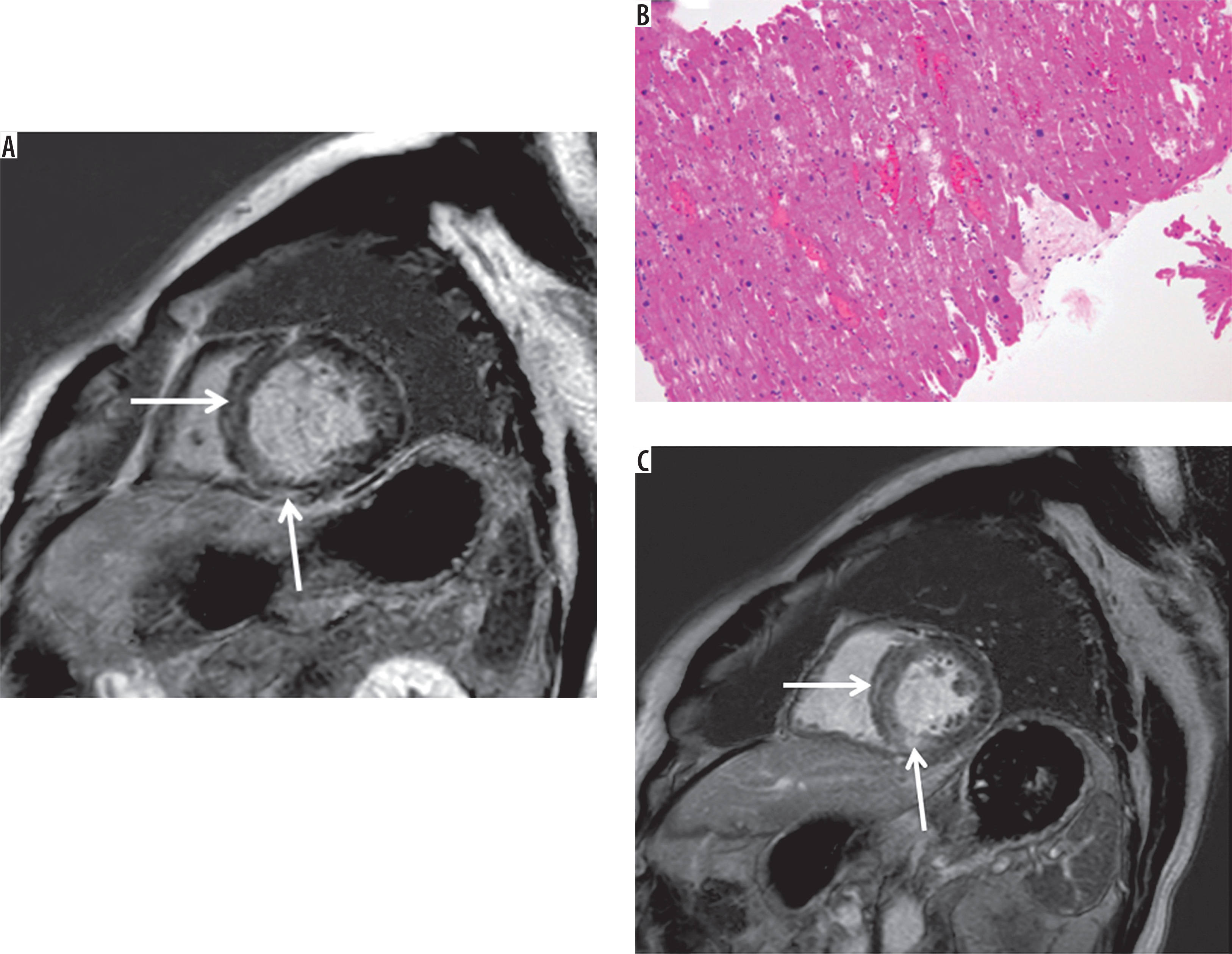
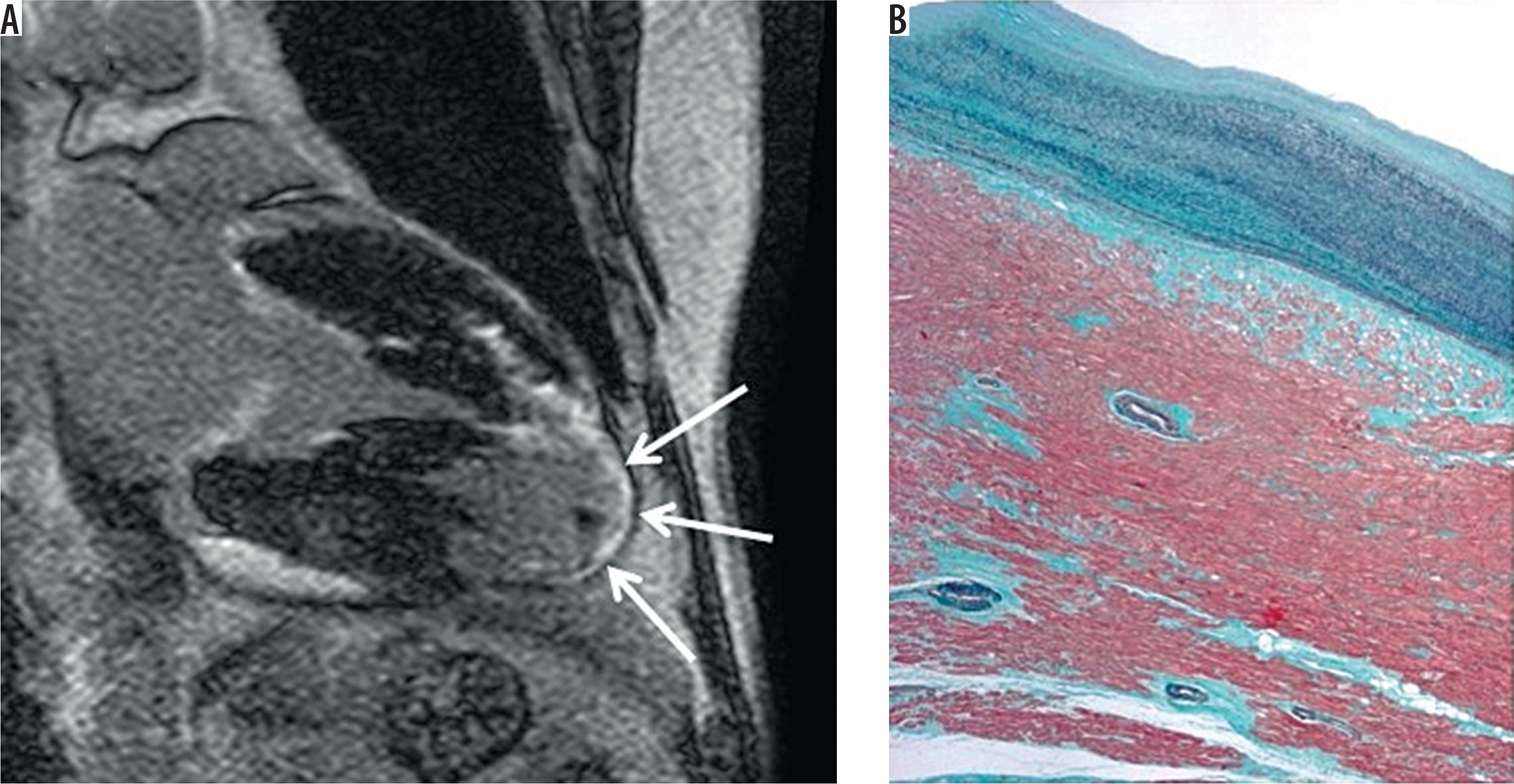
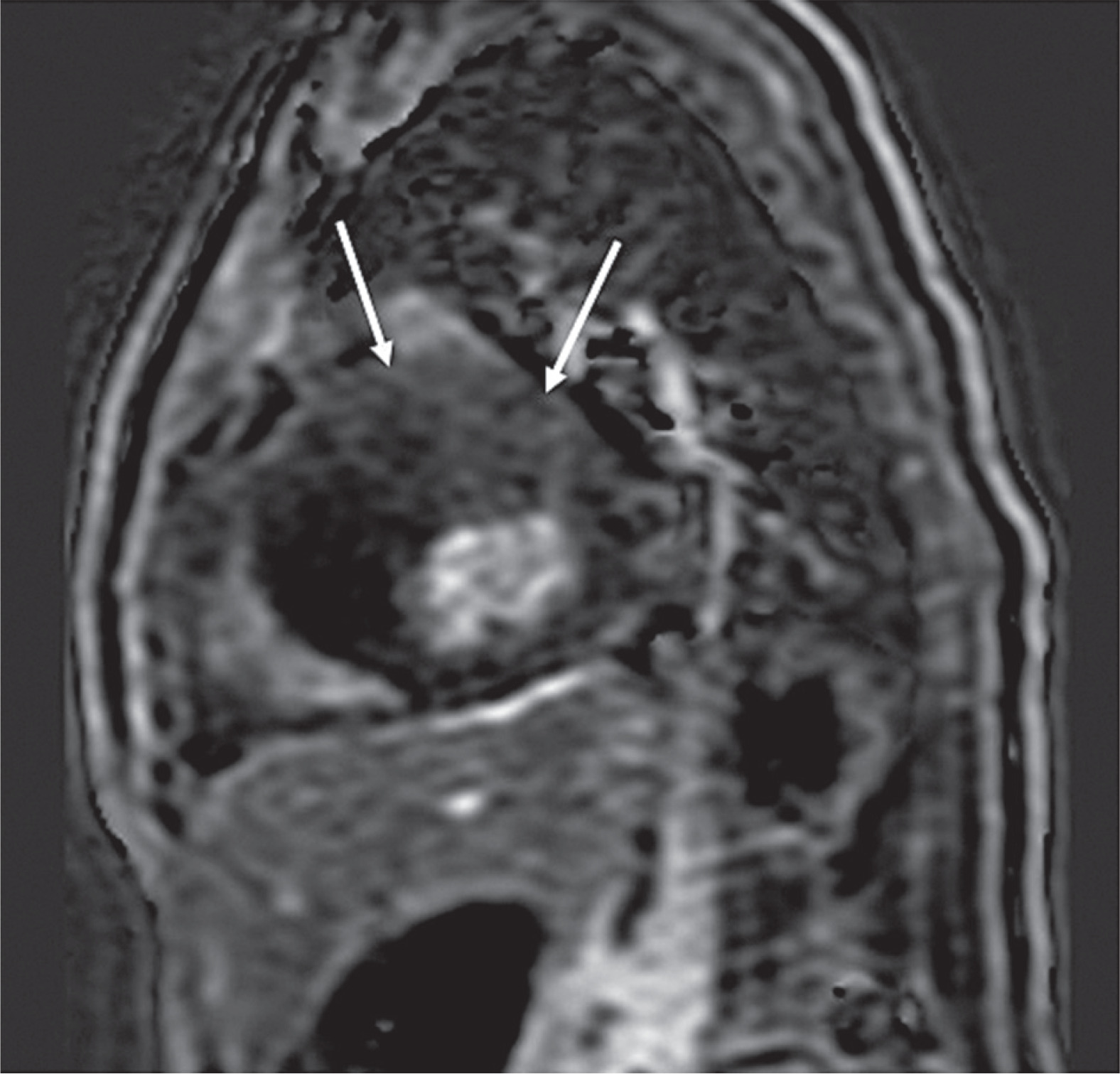
HHD is one of the leading causes of LVH and is often observed in older men who present with acute decompensated heart failure in the winter [18]. By contrast, concentric LVH and HFpEF induced by hypertension are commonly investigated in older women [23]. Obesity, diabetes mellitus, and sleep apnea syndrome are often associated with HHD. Cine SSFP reveals concentric LVH with a maximum LV wall thickness up to 16 mm in most patients with HHD [4,37,38]. Myocardial strain derived from cine SSFP or ECV correlates with the severity of LVH in HHD patients [9]. Approximately half of patients with HHD exhibit ischemic or non-ischemic LGE, whereas the remaining half of HHD patients lack LGE [32,39]. Non-ischemic LGE is observed at the inferior or septal myocardium at the basal or mid-ventricular level (Figure 1A) [32]. Cardiac MRI findings can be consistent with myocyte enlargement with slight fibrosis and no disarray in HHD patients (Figure 1B). The degree of LVH is proportional to systolic pressure; thus, successful anti-hypertensive treatments may lead to regression of LVH associated with HHD (Figures 1A, C) [1,38].
Figure 1
Hypertensive heart disease showing mild left ventricular myocardial hypertrophy and cavitary dilatation. A) Linear late gadolinium enhancement (LGE) is observed in the interventricular septum and inferior wall at the midventricular level (arrows). B) Endomyocardial biopsy reveals myocyte enlargement with slight fibrosis (hematoxylin and eosin staining). Myocardial disarray is not found. C) The left ventricular cavity regresses following anti-hypertensive treatments, whereas LGE remains (arrows)
HCM
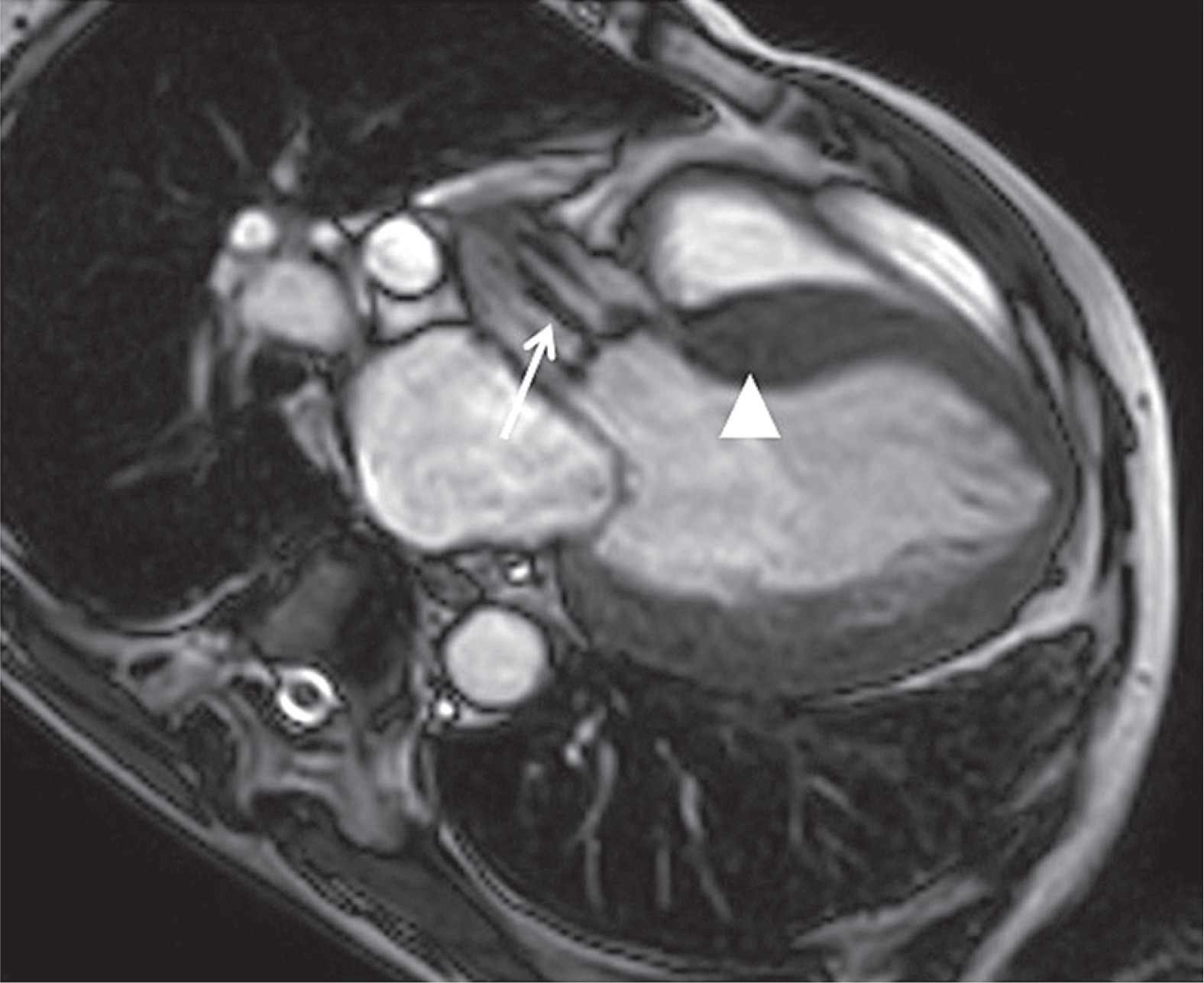
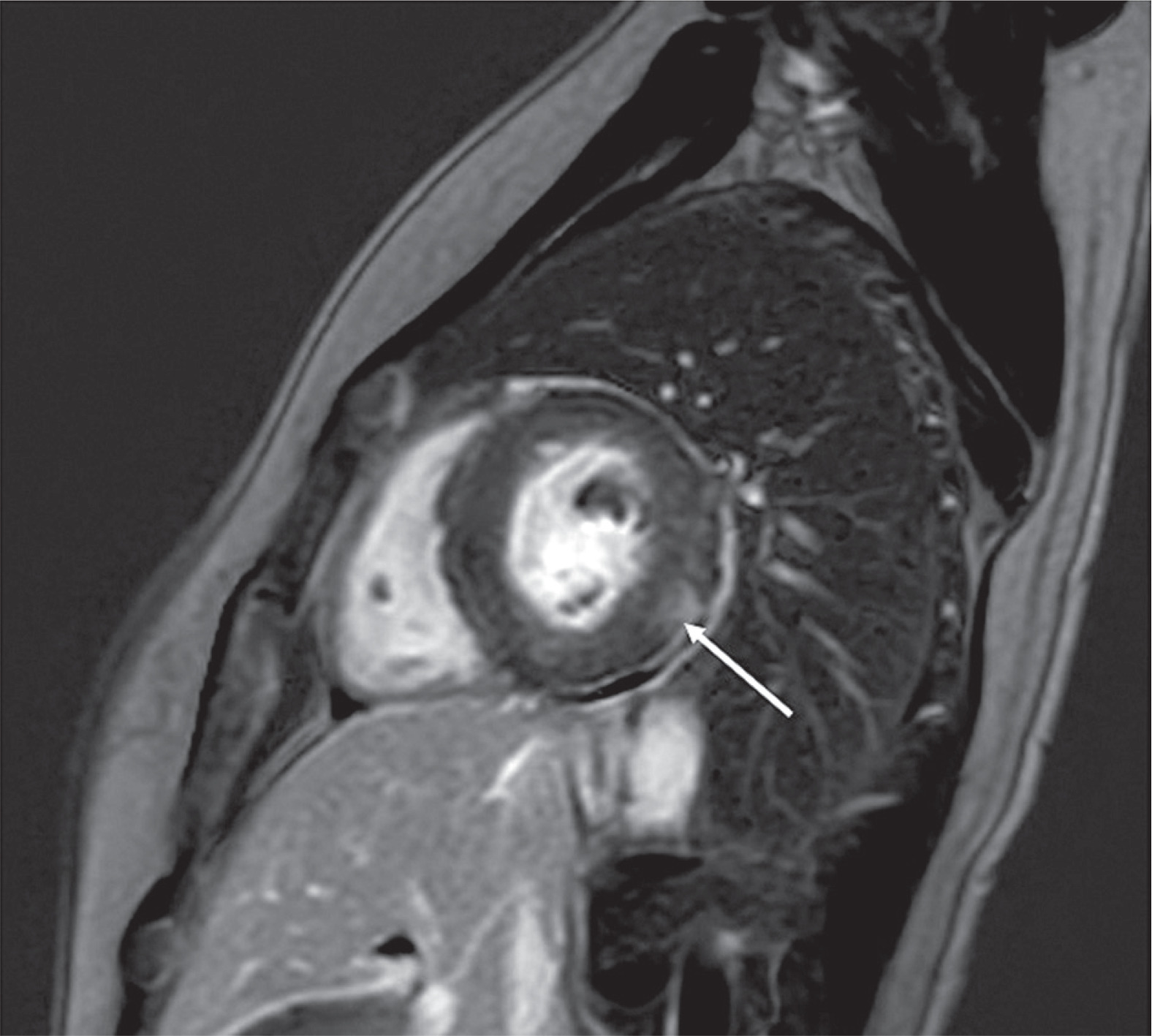
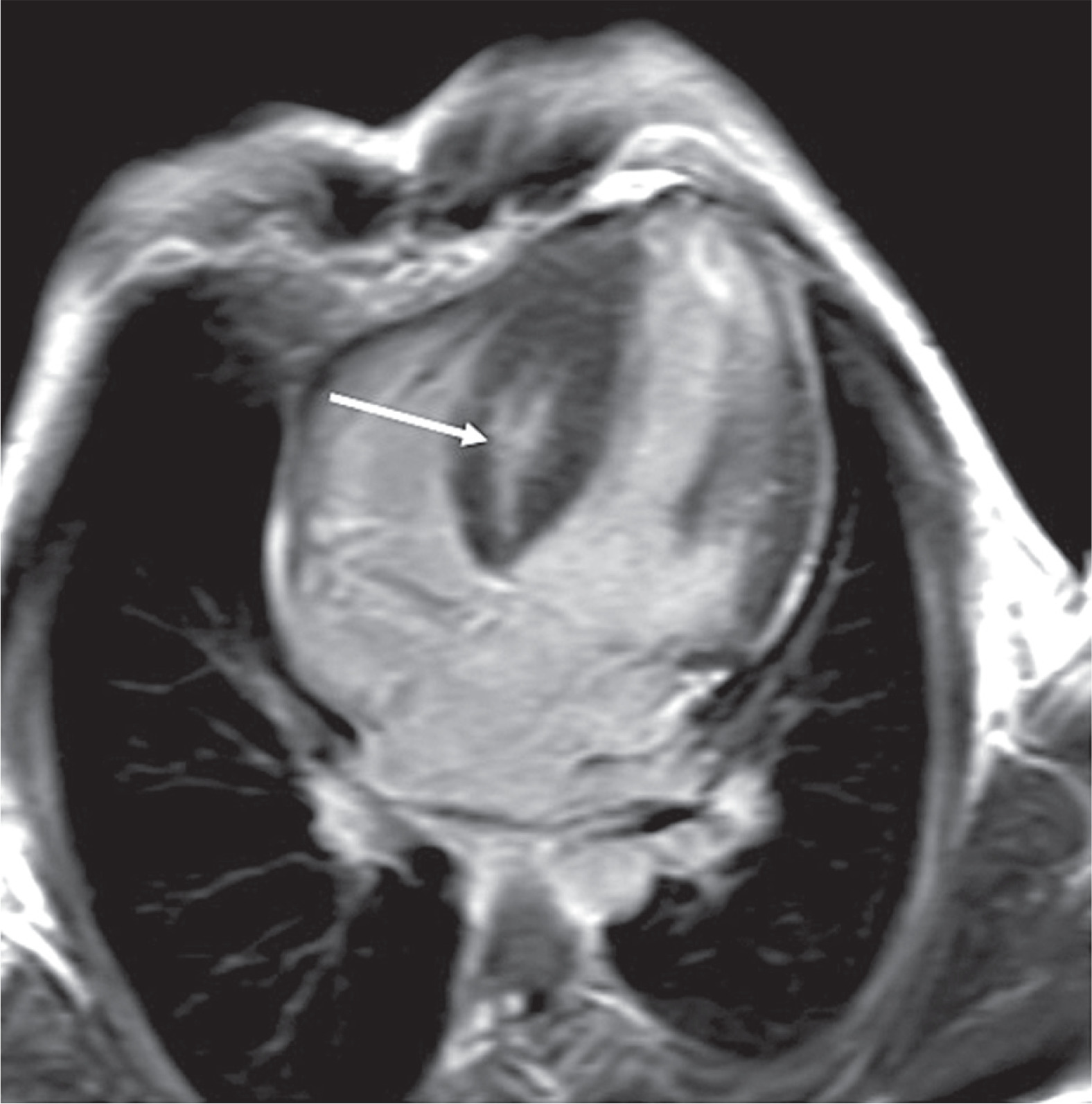
HCM is the most common primary cardiomyopathy, with causative genes observed in 1 case per 200-500 individuals in the general population [26]. While HCM has an autosomal dominant inheritance pattern, it is found more often in men than in women, probably because of high disease penetrance in male patients with cardiac myosin-binding protein C3 gene variants or modifier genes on sex chromosomes [22,40]. By contrast, HOCM is often observed in older women [10,22]. These patients with HOCM have isolated basal septal hypertrophy with a minimal family history of HCM, are negative for sarcomere mutations, and have less frequent LGE (Figure 2A) [41]. Cardiac MRI reveals structural and functional findings characteristic of HCM, including asymmetrical septal hypertrophy, midventricular obstruction, apical hypertrophy, and their combination (Figure 2) [2,27,28,36]. Hypertrophy of the papillary muscles, mitral valve elongation, myocardial crypt, and turbulence across the LVOT are investigated in patients with HCM (Figure 3A) [27]. HCM commonly shows LGE at the insertion point of both ventricles (Figure 3B) [7,27,31-33,36]. Stachera et al. [36] reported that cardiac MRI reveals HCM from the early to advanced stages, which may be related to the patients’ symptoms and prognosis. Importantly, cardiac MRI can identify high-risk HCM because it evaluates cardiac function (e.g., end-stage HCM) and the severity of LVH (e.g., maximum wall thickness ≥ 30 mm) and visualizes the presence, location (e.g., apical aneurysm), and extent (e.g., ≥ 15%) of myocardial scarring (Figure 4) [5,14,26,33,36,42]. ICDs should be installed in patients with high-risk HCM [5,41]. T2 reveals myocardial edema or vessel dilatation as high intense regions, possibly related to syncope, chest pain, and ventricular arrhythmia (Figure 3A) [29]. Cardiac MRI is now used to monitor cardiac structure of HOCM treated by recently developed cardiac myosin inhibitors [13].
Figure 2
Typical cine images of hypertrophic cardiomyopathy. A) Basal septal hypertrophy is observed at the end-diastolic phase, which evokes obstruction of the left ventricular outflow tract (arrow). B) Cine images at end-systole showing a midventricular obstruction (arrowhead) with an apical aneurysm (arrow). C) Apical hypertrophy is found at the end-diastolic phase (arrows)
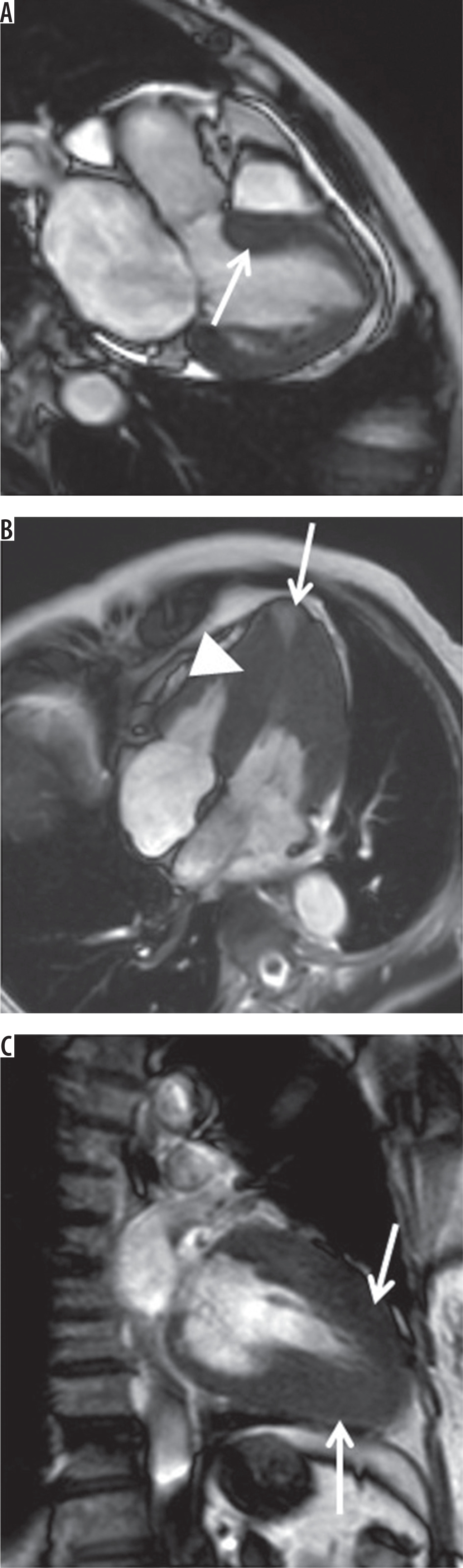
Figure 3
T2-weighted imaging reveals high intensity at the hypertrophied septum, which is related to unexpected syncope in this patient (arrows). The papillary muscle is also hypertrophied (arrowhead). B) Late gadolinium enhancement reveals typical myocardial scarring at the insertion point of both ventricles (arrows)
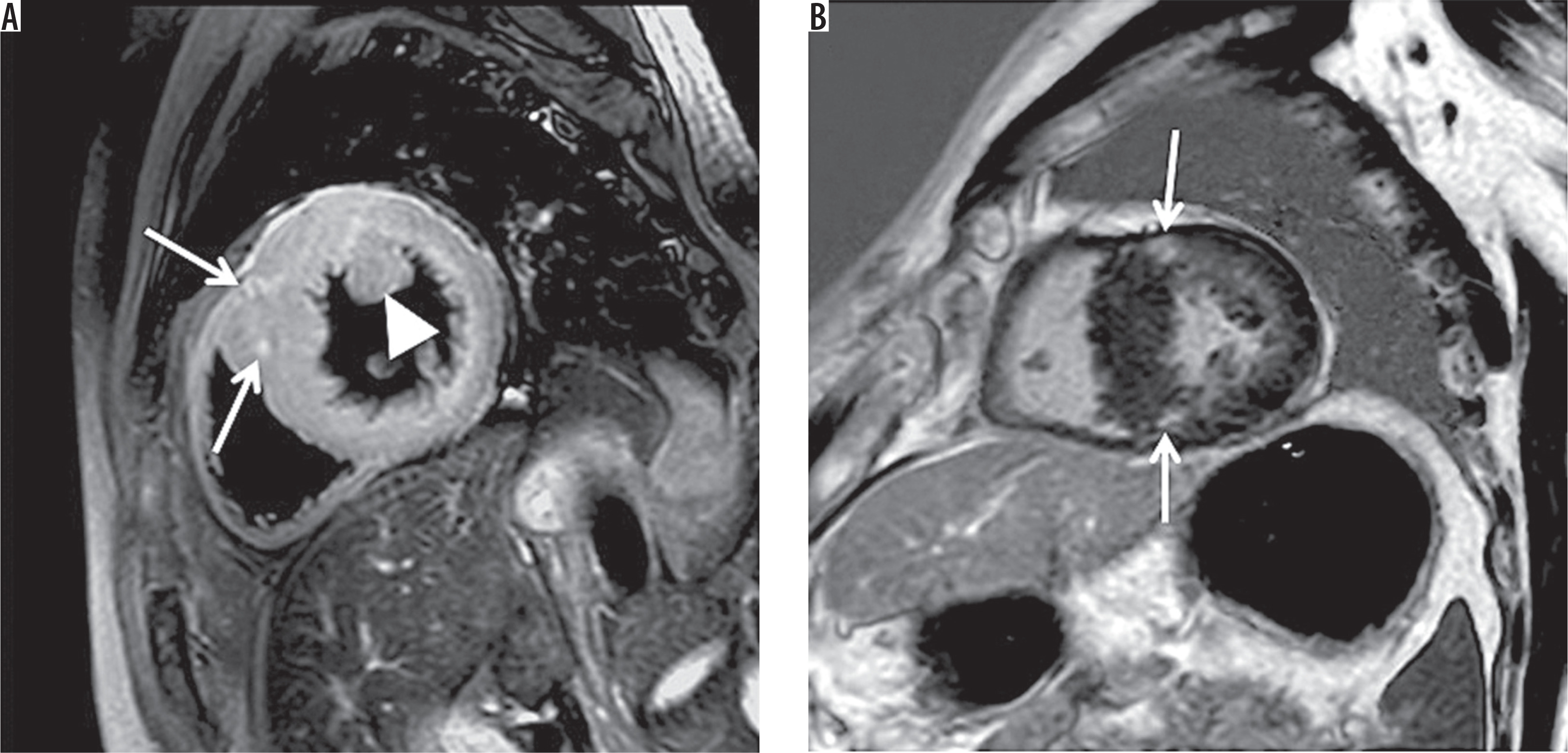
Figure 4
A) In midventricular obstructive hypertrophic cardiomyopathy (MVO HCM), transmural late gadolinium enhancement is observed at the apical aneurysm with a thin myocardial wall (arrow). B) Masson trichrome staining reveals marked replacement fibrosis at the resected apical aneurysm in another patient with MVO HCM
Aortic stenosis
Aortic stenosis is observed in elderly patients with and without a history of rheumatic fever and in middle-aged patients with bicuspid aortic valves. Because of the increase in afterload pressure, LVH occurs in patients with aortic stenosis (Figure 5). Echocardiography is the first-line method for evaluating aortic stenosis, and computed tomography is used to plan transcatheter aortic valve replacement. Lee et al. [43] demonstrated that T1 mapping is superior to LGE in predicting the prognosis of patients with aortic stenosis. Cardiac MRI is also useful for detecting concomitant cardiac amyloidosis in patients with aortic stenosis, in whom aortic valve replacement is far less effective than in patients with aortic stenosis alone [44].
Amyloidosis
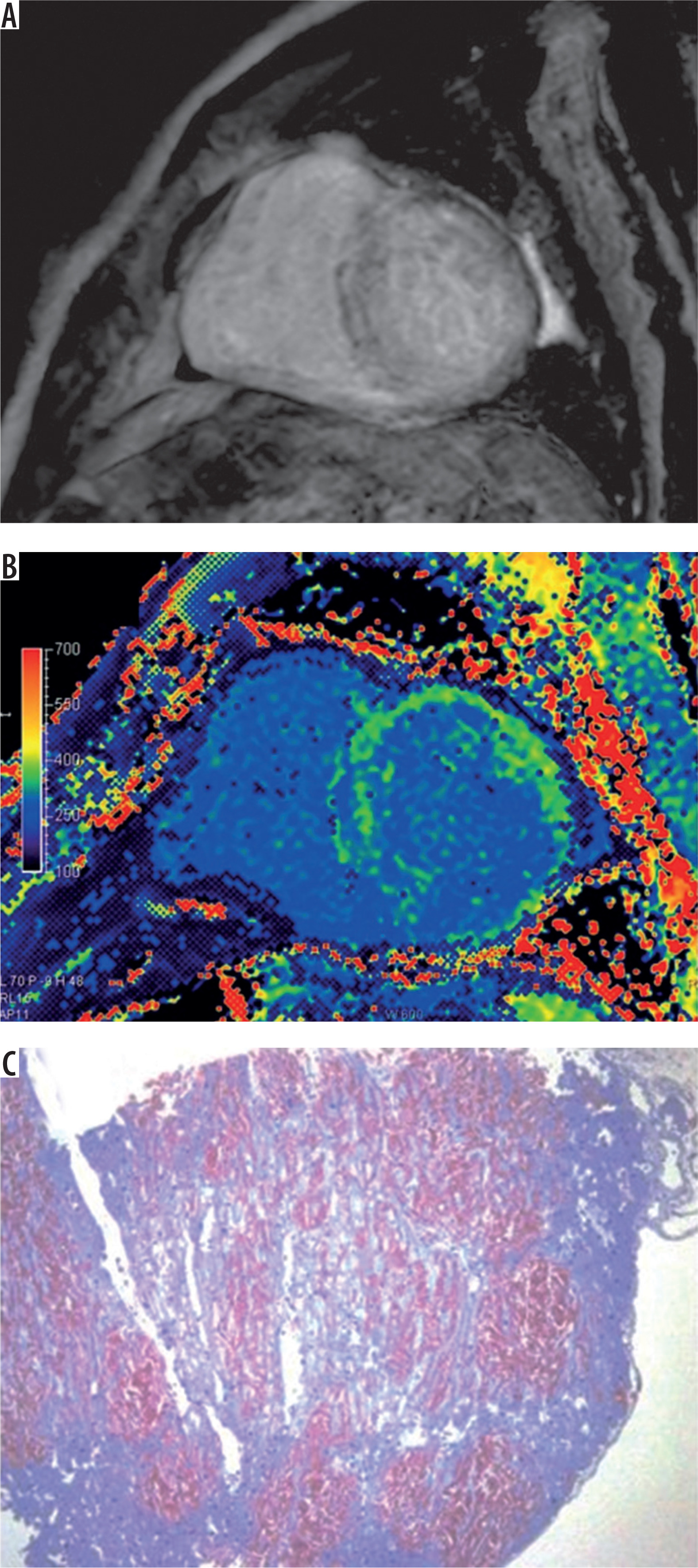
Cardiac amyloidosis is the second most common cardiomyopathy associated with LVH [2]. Wild-type ATTR amyloidosis is commonly observed in older men. Cardiac amyloidosis is characterized by LVH associated with HFpEF, low voltage on electrocardiogram, apical sparing on echocardiography, and pericardial and pleural effusion [1,19]. A noncardiac past history of carpal tunnel syndrome, lumbar spinal canal stenosis, abnormal immunoglobulin, or malignancies alerts us to amyloidosis. Cardiac MRI identifies LVH and pericardial and pleural effusion by cine imaging, as does marked dilatation of extracellular spaces by LGE and T1 mapping (Figure 6) [11,30,44,45]. The low contrast between the LV myocardium and blood in the LV cavity after contrast enhancement is characteristic of cardiac amyloidosis (Figures 6A, B) [1,45].These MRI findings help differentiate between cardiac amyloidosis and other etiologies of LVH. Cardiac MRI is also used to monitor the response of cardiac amyloidosis to chemotherapy and ATTR stabilizers. Tafamidis improves ventricular function, whereas ECV and T1 values do not change after tafamidis treatment in a non-randomized single-center study [11].
Figure 6
A) Cardiac amyloidosis shows diffuse late gadolinium enhancement. B) The postcontrast T1 value of the septal myocardium at 300 ms is close to the blood T1 value of 290 ms. The extracellular volume fraction is markedly elevated at 51.9% (> 28.0%, the upper limit of the reference value). C) Direct fast scarlet staining reveals diffuse distribution of amyloid fibrils (bright brown)
Anderson-Fabry disease
Anderson-Fabry disease is a relatively rare, X-linked lysosomal storage disease caused by mutation of genes encoding α-galactosidase. Pain in the extremities, hypohidrosis, and premature stroke were reported to precede LVH, followed by renal impairment [21,34]. In some heterozygous women affected by this disease, symptoms may be limited to the heart [21]. Previous studies revealed that LVH is significantly related to heart failure and critical ventricular arrhythmias in this disease [34,46]. Glycosphingolipids accumulate progressively in the heart, which leads to a shortened myocardial T1 value. Therefore, native T1 mapping is valuable for distinguishing Anderson-Fabry disease from other etiologies of LVH that show normal or prolonged T1 (Figures 7A) [1,2,21,30,46]. A pathological study revealed sarcoplasmic vacuolization reflecting glycosphingolipid accumulation in myocytes, fatty infiltration, and myocardial fibrosis, which are consistent with cardiac MRI features [47]. Myocardial LGE at the lateral to inferolateral wall at the basal level is characteristic of Anderson-Fabry disease (Figures 7B) [31,47]. The location of LGE may be attributed to higher mechanical stress, greater energy demand, or abundant mitochondria in the basal inferolateral region [46]. Although myocardial T1 is reduced in Anderson-Fabry disease, myocardial fibrosis induces pseudo-normal or prolonged T1 [48]. Cardiac MRI shows improvement in LVH after enzyme replacement therapy in affected patients [12].
Mitochondrial myopathy
Mitochondrial myopathy is maternal, autosomal dominant, or recessive in nature. This disease often involves the heart as well as the cerebellum and skeletal muscles. Interestingly, mitochondrial myopathy is characterized by intramural or transmural LGE at the inferolateral myocardium, as found similarly in Anderson-Fabry disease (Figure 8) [25]. Yilmaz et al. [25] reported that this disease predominantly involves aggregates of mitochondria in the basal inferolateral wall subject to higher mechanical stress.
Glycogen storage diseases
Glycogen storage diseases are rare metabolic disorders caused by a deficiency of enzymes or transporters related to glycogen metabolism. Glycogen storage disease type IIIa is inherited in an autosomal recessive manner and involves the heart [15]. Cardiac MRI shows marked hypertrophy and LGE at the septum in this disease (Figure 9) [2,15]. Excessive glycogen accumulation in the conduction system and interstitial space of the heart leads to atrioventricular block and myocardial scarring, respectively.
Noonan syndrome
Noonan syndrome is inherited in an autosomal dominant or sporadic manner. Intellectual disabilities and body appearances allow a diagnosis of Noonan syndrome, whereas it shows cardiac MRI findings similar to those found in pediatric HCM, including marked septal hypertrophy and anterior to septal LGE (Figure 10) [16]. Myocardial involvement is a predictive of the prognosis of Noonan syndrome.
Chronic kidney disease
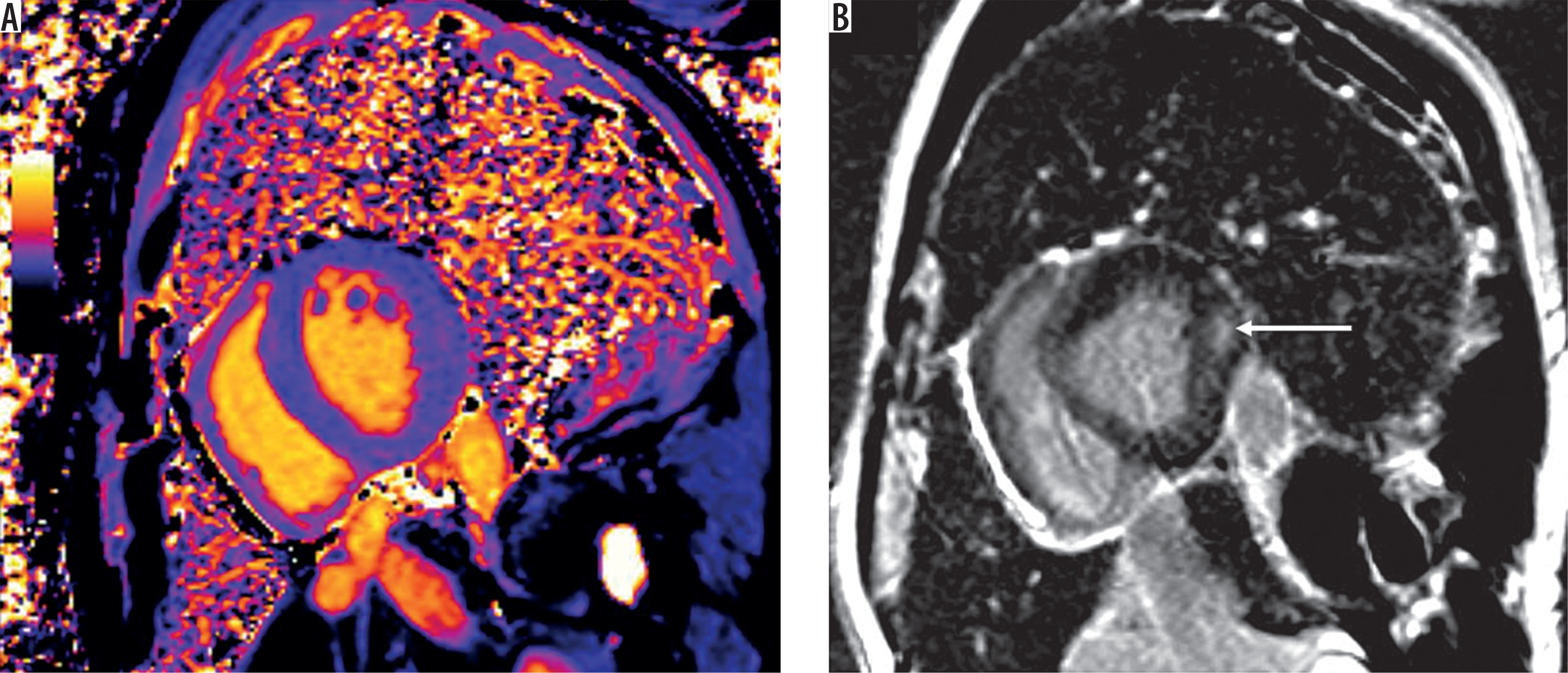
Chronic kidney disease (CKD) leads to LVH and is associated with HFpEF [18,23]. Hayer et al. [49] reported that native T1 increases incrementally from stages 2 to 5 of CKD independently of hypertension (Figure 11A), while Arcari et al. [50] observed that the T2 value increases significantly in patients with CKD but not in those with HCM or HHD (Figure 11B). Increased T1 and T2 of the myocardium may reflect interstitial fibrosis and water overload, respectively. LV wall thickness may be significantly greater in patients with CKD than in those with HHD [1]. CKD is significantly related to coronary artery diseases as well as congestive heart failure or SCD. Cardiac MRI aids in the risk stratification of CKD by assessment of LVH and myocardial fibrosis (Figures 11A, C) [51].
Figure 11
A) Chronic kidney disease exhibits an increased T1 of 1127 ms (> 1110 ms, the upper limit of the reference value) and B) T2 of 55 ms (> 51 ms, the upper limit of the reference). C) An autopsy of another patient with CKD reveals marked fibrosis intervening in the myocardial layers (Masson trichrome staining)

Comorbidities of etiologies presenting LVH
HCM and athletic LVH are well-known comorbidities, especially in adolescents presenting with SCD [20]. Unexpected SCD can occur during or immediately after physical activities, including marathons, soccer, basketball, and football, and can be an initial symptom in young competitive athletes with HCM. Compared with athletes’ LVH, HCM tend to have a thicker myocardium, smaller LV cavities, asymmetrical LVH, and diastolic dysfunction [1,52]. HCM and HHD are comorbid pathologies in middle-aged to older patients. While both HHD and HCM present with LV myocardial wall thickness greater than 13-15mm, HCM tends to have a thicker myocardium (e.g., > 16 mm) and asymmetrical LVH than HHD [1,37,38]. The LGE pattern differs between HHD and HCM with hypertension [31,32,39]. The family history of HCM also helps distinguish HCM from HHD. Nonetheless, it can be difficult to distinguish HCM from HHD when patients with HHD exhibit marked LVH > 16 mm [38,40]. Hypertension, obesity, and competitive sports are reported to be associated with penetrance and phenotypic expression of HCM [24,40,52]. LVH regression after anti-hypertensive treatments should be assessed in patients with LVH and hypertension [38]. Adequate use of beta-blockers and calcium antagonists may be crucial in patients who are suspected to have both HCM and hypertension, before initiating class Ia anti-arrhythmic agents, cardiac myosin inhibitors, or interventional procedures [11,13,38,40,53,54].
In older patients, aortic stenosis and cardiac amyloidosis can coexist. Low flow and low gradient across the LVOT or marked LVH on echocardiograph can indicate the comorbidities of aortic stenosis and amyloidosis. LGE helps identify amyloidosis in patients with aortic stenosis [44]. The prognosis is worse in patients with both aortic stenosis and cardiac amyloidosis than in those with aortic stenosis alone, even after aortic valve replacement [44].
CKD is often associated with hypertension and possibly HHD. A previous report suggested the usefulness of cardiac MRI for determining the etiology of LVH, whether CKD or HHD [50].
Conclusions
LVH is commonly encountered in patients presenting with chest pain, HFpEF, and cardiac arrest. LVH is caused by a wide variety of myocardial diseases. Cardiac MRI is useful for determining the etiologies of LVH and stratifying their risks for heart failure and cardiac death in patients with LVH. Of note, its utility is enhanced by combining clinical information, including patient’s age, and family history in patients with LVH. Among the sequences, LGE has a pivotal role in cardiac MRI of LVH.