Introduction
Foetal alcohol spectrum disorder (FASD) is a broad term describing a range of conditions that may be caused by prenatal exposure to alcohol [1]. It comprises such diagnostic terms as:
foetal alcohol syndrome (FAS) (Q 86.0), a condition in which the child presents at least 3 primary dysmorphic features specific to foetal alcohol exposure and at least 3 dysfunctions associated with the central nervous system (CNS), including impaired functioning;
partial foetal alcohol syndrome (pFAS), a condition in which there are fewer than 3 facial dysmorphic features and fewer than 3 dysfunctions of the CNS;
alcohol-related neurodevelopmental disorder (ARND), a condition in which a child presents neurodevelopmental deficits linked to prenatal alcohol exposure. There may be no facial dysmorphic features.
A meta-analysis of research focusing on the intelligence of children with FASD, conducted in 2017, took into account 37 articles [2]. The authors of the review pointed out that the findings are not clear and consistent. While some studies reported a reduced IQ in children with FASD, others showed that children in this group may have a normal IQ. However, all studies point to difficulties in the functioning of children in this population [3]. These include intellectual deficits, executive dysfunction, problems related to memory and learning, impairment in speech and language development, particularly affecting verbal fluency and the capacity to understand the meta context of language, visuospatial deficits, problems related to delayed motor development, and attention deficits, as well as adaptive, emotional, and social difficulties. If they receive insufficient care and no support, individuals with FASD may experience secondary disorders reflected in problems related to education, general health, or legal issues [4,5].
Difficulties in functioning and low IQ in children with FASD may be linked to changes in brain structures [6,7], particularly in the frontal lobes [1,8,9]. This may be attributed to the fact that the frontal lobes play a role in many processes, including cognitive and other complex mental functions [10,11]. The upper part of the frontal lobe controls motor functions, whereas its left lobe comprises the Broca area responsible for speech. It also contains the prefrontal cortex, responsible for higher brain functions related to intellect, planning, motivation, and controlling emotional states. An earlier study of 200 children with FASD showed metabolic changes in this area [12].
The aim of this study is to assess the relationship between the metabolism in the frontal lobes of the brain and the IQ in children with FASD, using proton magnetic resonance spectroscopy (1H-MRS).
Material and methods
The study assessed a total of 124 children of both genders, aged 5-17 years, with diagnosed FASD, including 62 children with FAS, 34 children with pFAS, and 28 children with ARND. The control group consisted of 32 healthy children of both genders (aged 6-19 years, mean 12.53 years) with no history of FASD or craniocerebral trauma, and taking no medication. Children came for the assessment from all over Poland. Approval for the study was obtained from the local Bioethics Committee in accordance with the Declaration of Helsinki. The parents or legal guardians of each participant gave their voluntary informed consent for their child to participate in the study.
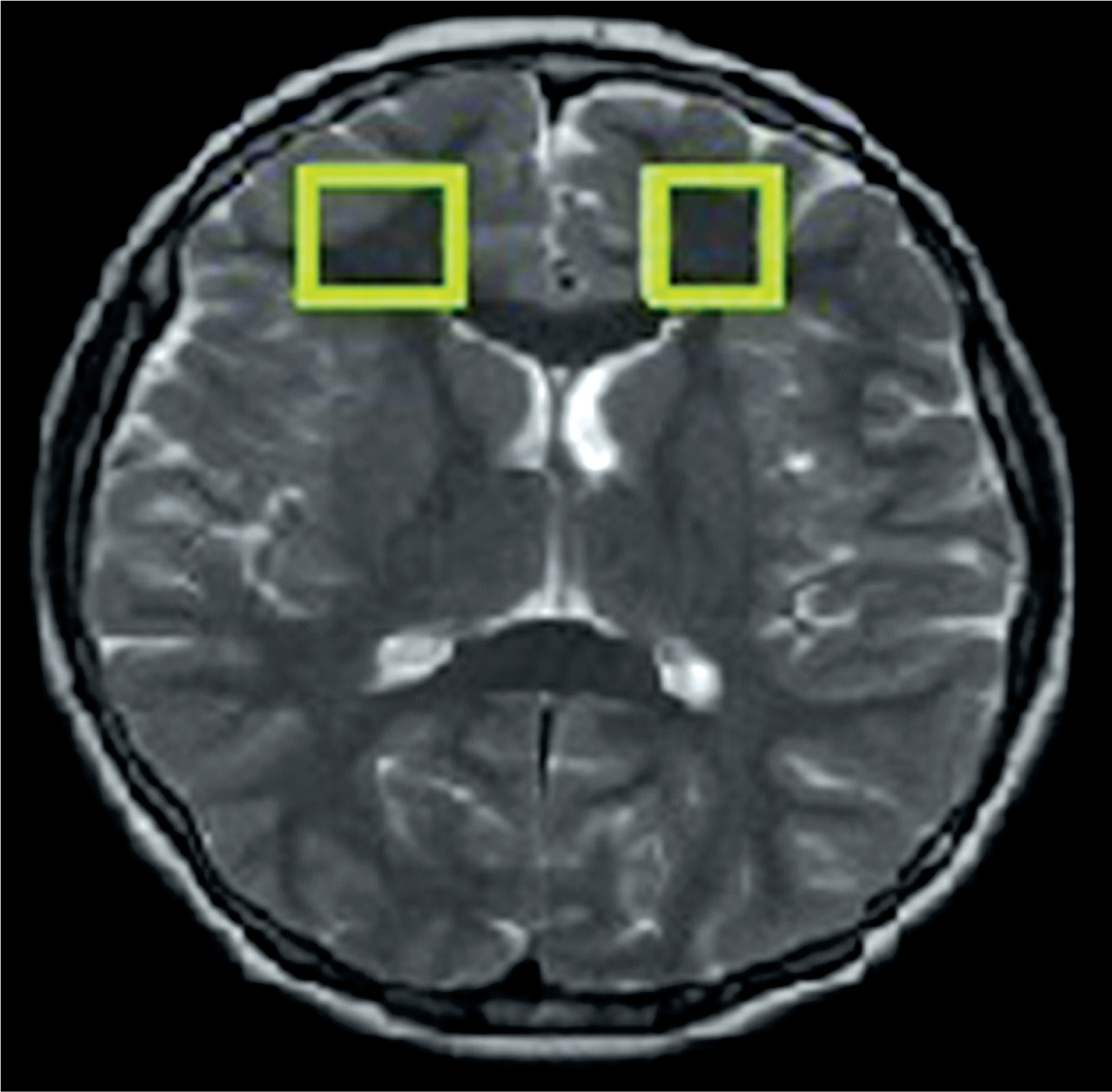
The examinations were performed with MR Signa HDxt 1.5 T (GE) using a transceiver head coil. The 1H-MRS was carried out using the Point-Resolved Spectroscopy Sequence (PRESS) method (TE = 35 ms, TR = 1500 ms, number of acquisitions = 128, slice thickness = 20 mm). Spectroscopic signal was acquired from volumes of interest (VOIs 2 × 2 × 2 cm) in the left and right frontal lobes (Figure 1). A quantitative analysis of the spectroscopic data was performed using SAGE 7.0 dedicated software (Spectroscopy Analysis, GE). Concentrations of the specific metabolites (N-acetylaspartate – NAA, choline – Cho, myo-inositol – mI, lipids – Lip, lactates – Lac) were determined in relation to the concentration of creatine (Cr). Moreover, the mean concentration values were calculated for each hemisphere, then the concentrations in both hemispheres were added, and the total was divided by 2.
Figure 1
Volume of interest localised in the frontal lobe symmetrically in the right and left hemispheres
Assessment of the study participants’ intelligence was performed using the Wechsler Intelligence Scale for Children (WISC-R ) by an experienced clinical psychologist in a psychological counselling centre. During the diagnostic process, to verify finally the FASD diagnosis, information about the child’s developmental history was acquired from their parents (they filled in a questionnaire about the child’s growth). Subsequently, a complex assessment of the child was performed using the Berry-VMI test, clinical trials from the RHLB-PL battery, a verbal fluency test, and neurodevelopmental examination.
The differences between healthy children and children with FASD in Full Scale IQ scores and metabolite concentrations in the frontal lobes of the brain were examined using Student’s t-test and, if the condition for homogeneity of variance was not met, the Mann-Whitney U-test was applied. The differences in IQ scores acquired by the controls and the subgroups of children with FAS, pFAS, and ARND were determined using one-way ANOVA and verified using a post-hoc Bonferroni test. The Pearson correlation was applied to measure the linear relationship between IQ scores and the relative concentrations of the specific metabolites in the frontal lobes of the brain in the children with FASD and the controls. The results were assumed to be statistically significant if p < 0.05.
Results
IQ scores in children with FASD and in the control group
In the IQ tests, all children with FASD obtained IQ scores in the range 41-133 (mean 90.42). The controls had IQ scores of 97-142 (mean 121.26). There was a statistically significant difference in IQ scores between the group of children with FASD and the control group (p < 0.01). A comparative analysis performed using ANOVA test did not show statistically significant differences in the scores between the subgroups of children with FAS, pFAS, and ARND (p > 0.05). There was only a statistically non-significant trend towards a lower IQ in the subgroup of children with FAS (Figure 2). The IQ scores in the specific subgroups (control group, FAS, pFAS, ARND) are shown in Table 1.
Table 1
Respective values of IQ in children with foetal alcohol spectrum disorder (FASD) and in the subgroups of children with foetal alcohol syndrome (FAS), partial foetal alcohol syndrome (pFAS), and alcohol-related neurodevelopmental disorder (ARND)
| IQ value | Control (n = 52) | FASD (n =124) | FAS (n = 62) | pFAS (n = 34) | ARND (n = 28) |
|---|---|---|---|---|---|
| Min | 97 | 41 | 41 | 55 | 55 |
| Max | 142 | 133 | 126 | 133 | 117 |
| Mean | 121.26 | 90.42 | 86.66 | 94.47 | 93.82 |
| Standard deviation | 11.07 | 18.03 | 18.70 | 17.16 | 16.30 |
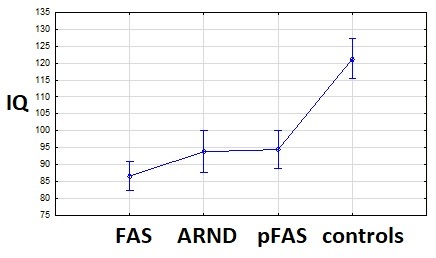
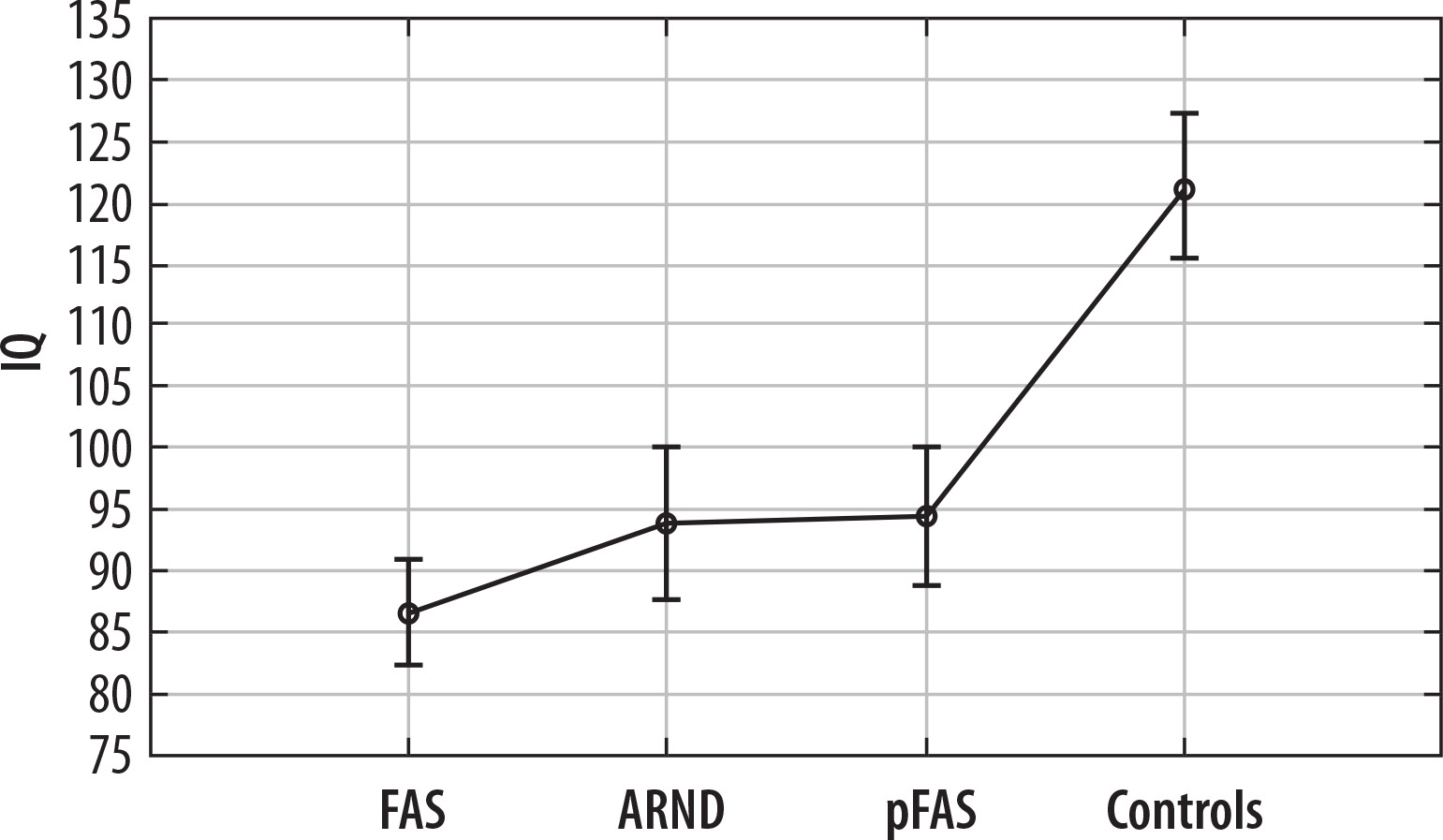
Figure 2
Comparison of IQ scores in the controls and the subgroups of children with foetal alcohol syndrome (FAS), partial foetal alcohol syndrome (pFAS), and alcohol-related neurodevelopmental disorder (ARND). Dots represent mean values, vertical bars indicate 0.95 confidence intervals
Because there were no statistically significant differences in IQ scores between the children with FAS, pFAS, and ARND, further analyses were conducted for the whole FASD group, without distinguishing these subgroups.
Comparison of metabolite concentrations in children with FASD and in the control group
The proton MR spectroscopy examinations provided information about metabolite concentrations in the frontal lobes of the brain in children with FASD and the controls. In the left frontal lobe, significantly higher Lip/Cr levels were observed in the children with FASD than in the controls. No other statistically significant differences in the concentrations of other metabolites were found. The results are listed in Table 2. A comparative analysis of the specific metabolite concentrations in the investigated locations showed no statistically significant differences in these values between the subgroups of children with FAS, pFAS, and ARND (p > 0.05).
Table 2
Comparison of metabolite concentrations in the frontal lobes in children with foetal alcohol spectrum disorder (FASD) and controls
Correlations between IQ scores and metabolite concentrations in children with FASD and in the control group
Tests were performed to determine the correlations between IQ scores and the relative concentrations of specific metabolites in the frontal lobes of the brain in children with FASD and in the controls. The findings show significant negative correlation between IQ scores and Lip/Cr concentrations in the right frontal lobe as well as in both frontal lobes in children with FASD. No statistically significant correlations were found between the other metabolites and IQ (Table 3). In the control group, no statistically significant correlations were found between metabolite concentrations and IQ. Likewise, in the combined group of children with FASD and children in the control group, no statistically significant correlations were found for metabolite concentrations and IQ scores.
Table 3
Correlations between IQ and metabolite concentrations in the frontal lobes in the foetal alcohol spectrum disorder (FASD) group
Discussion
IQ scores in children with FASD and in the control group
In the IQ tests performed in the current study, children with FASD acquired IQ scores in the range 41-133 (mean 90.42), whereas in the control group IQ scores were significantly higher, in the range 97-142 (mean 121.26). No significant differences in IQ scores were identified between children with FAS, pFAS, and ARND.
The results showing lower IQ in children with FASD are consistent with the literature related to this subject matter. Early studies focusing on children with FASD reported that IQs in this population are reduced. A study conducted in Sweden in 1985 by Aronson et al. [13] found that children born to alcoholic mothers showed lower IQs than children born to non-drinking mothers, by an average of 15-19 points. The latter study also reported differences between children with FAS and the control group related to other variables relevant to development. Children with FAS showed impaired visual perception, could not draw human figures correctly, had problems with emotional stability, and exhibited hyperactivity and attention difficulties – short attention span and perseveration adversely affected their task performance. None of these characteristics occurred in the healthy controls, although this group also included children raised in foster and adoptive families; in this case, purposive sampling was applied to exclude environmental factors contributing to the impairment of the abilities investigated. The 1985 study also found that the presence of physical symptoms of FAS correlated with lower IQ, which was consistent with earlier evidence related to this issue [13]. Furthermore, individuals diagnosed with FAS but presenting no features specific to FAS were also found to have IQs significantly lower than the controls. Thus, the conclusion was drawn that neurological and psychological impairment can also occur when the distinctive dysmorphic features are not present.
Research conducted in Europe in the 1990s by Professor Hans Ludwig Spohr from Germany contributed new evidence related to the functioning of children with FAS. Long-term effects and developmental consequences were observed in 60 children diagnosed with FAS in infancy or early childhood [14]. As for IQ tests, the results ranged from low scores reflecting disability to above average values. This suggests that assessment of intelligence has a limited diagnostic value, because this measure does not effectively identify differences in the difficulties and impairments exhibited by this diverse group of children [13]. When IQ scores of children with pFAS and ARND were compared, there were no differences between these subgroups, and the overall IQ was lower than in the control group. In contrast, factor analysis of the results in the Weschler test showed that children with FAS had significantly lower scores than children in the pFAS and ARND subgroups, whereas the pFAS and ARND subgroups did not differ. The present study showed no statistically significant differences in IQs between the groups of children with FAS, pFAS, and ARND.
Lower IQ in children with FASD may be directly linked to the deficits in their cognitive performance. Executive functions include the higher-order processes involved in decision-making and planning related to the task at hand [15]. Important in these processes are the abilities to act in line with the intended goal. At their core is the ability to work out new patterns of behaviour and ways of thinking, as well as the ability related to the evaluation of these new patterns [16]. According to Muriel Deutsch Lezak, executive functions are also related to creative and abstract thinking, evaluation of one’s own needs or desires and the effectiveness of satisfying these, as well as evaluation of one’s own desires and the procedures for fulfilling these [16]. The findings of research focusing on executive function in individuals with FASD show that they have deficits in assessing and critically examining their own behaviour. Individuals with FASD can only process a limited amount of information, and this makes it difficult to plan a solution to a problem and to execute a plan [15]. A review of studies related to these issues in children with FASD has been published by Polish researchers [17]. The analysis showed that children with FASD may have a wide variety of executive function deficits. Children with FASD may exhibit difficulties resulting from deficits in inhibition and regulation, as well as related to working memory and cognitive flexibility. The meta-analysis cited here lacks data on the level of coping with multitasking situations by children with FASD; however, clinical practice shows that they have difficulties in continued performance of the criterion task.
Comparison of metabolite concentrations in children with FASD and in the control group
The proton MR spectroscopy examinations carried out for the present study showed metabolite concentrations in the frontal lobes of the brain in children with FASD and in the controls. In the left frontal lobe, significantly higher Lip/Cr concentrations were found in the children with FASD than in the controls, which is consistent with an earlier study carried out in a group of 200 children with FASD [12]. An increase in the concentration of this metabolite may be indicative of cell membrane damage. There are no more reports in the literature on changes in lipid concentrations in children exposed to alcohol during foetal life [18].
Likewise, there is a scarcity of studies reporting evidence related to other metabolites measured in the frontal lobes of children with FASD. Fagerlund et al. [11] found lower levels of NAA/Cho and NAA/Cr, and lower concentrations of Cho in children with FASD. Conversely, the current study found no other statistically significant differences in the concentrations of other metabolites (NAA/Cr, Cho/Cr, mI/Cr, Lac/Cr) in the frontal lobes between children with FASD and healthy controls.
Correlations between IQ scores and metabolite contents in children with FASD and in the control group
The present findings show a significant negative correlation between IQ scores and Lip/Cr concentrations in the right frontal lobe in children with FASD. However, in the case of the left frontal lobe there is an analogous tendency (p < 0.1). Also, while analysing both frontal lobes together, a significant negative correlation between IQ scores and Lip/Cr concentrations is observed. It is necessary to emphasise here that the direction of dependencies is the same in both hemispheres. Only the degree of their intensity differs. Given that a higher level of this metabolite may be indicative of damage to the neuronal cell membrane, it may lead to lower IQ. It should be noted that both structural and functional brain asymmetries are observed especially in the early phases of life. This may explain the differences in the degree of statistical significance of the results obtained between the hemispheres. This problem is explained in an article by Bisiacchi and Cainelli [19]. The results of this work are also confirmed by the description of twins who were exposed to alcohol to the same extent in the prenatal period but showed different spectra of disorders [20].
Correlations between IQ values and metabolite concentrations have been reported in a limited number of studies, which predominantly focused on healthy adults. To the best of our knowledge, a few research teams have investigated this issue in children, but no one has focused specifically on children with FASD. Deng et al. [21] observed a positive correlation between NAA/Cr concentrations and IQ in girls with idiopathic central precocious puberty. A study involving children with Down syndrome showed a positive correlation between IQ and NAA/Cr in the frontal lobes but in no other investigated metabolites (Cho, mI) [22]. On the other hand, no statistically significant correlations between IQ and levels of NAA/Cr in the frontal lobes were found in children with autism spectrum disorder in a study by Fujii et al. [23].
In healthy adults, Jung et al. observed a positive correlation between IQ and NAA as well as Cho concentrations in the left occipitoparietal white matter [24,25], as well as NAA concentration in the right anterior grey matter [26]. Likewise, a positive correlation has been reported between IQ and NAA concentrations in the corpus callosum [27]. Some researchers have demonstrated gender differences regarding this issue. According to Pfleiderer et al. [28], NAA levels in the left frontal cortex are associated with verbal intelligence in adult females but not in males. Jung et al. [25] reported a similar finding with respect to the left frontal lobe and the left occipitoparietal lobe.
Study limitations
The current study has certain limitations. The subject of the study is extremely important due to the retrospective analysis of limited information given on timing and duration of alcohol consumption during pregnancy. Moreover, the development of the frontal lobes is intricate and protracted over time. It would be desirable to evaluate the IQ of children with FASD and that of healthy children in terms of metabolism assessed by the 1H-MRS technique in longitudinal through the years of growing up.
Conclusions
Children with FASD have a significantly lower IQ than their peers from a healthy control group. This may be linked to the changes in the frontal lobes, in particular the elevated lipid levels. A negative correlation was observed in the group of children with FASD between the concentration of this metabolite and IQ: higher IQ in a child with FASD corresponded to lower lipid concentration.