Introduction
In recent years, tractography has become a key and very important technique for imaging white matter fibers, especially prior to the planning of neurosurgical procedures. By quantifying the anisotropic diffusion of water molecules, it enables the reconstruction of white matter pathways in vivo [1]. Initially a research tool, tractography now bridges the gap between basic neuroscience, neuroanatomy, and clinical practice. It is used not only to plan operations, but also to study brain connectivity, validate neuroanatomical models, and understand how white matter supports cognitive and behavioral processes. Currently, tractography is the only imaging method that allows for indirect, non-invasive, and spatial visualization of the position, course, and projection of nerve fibers of white matter. This method has been widely used in neurosurgery and neurology, and is a valuable tool in scientific research. With this technique, it became possible to map white matter pathways to identify previously unknown projections [2].
Initially, tractography was considered primarily a research tool; however, the rapid development of computer technology and the increased availability of high field magnetic resonance imaging (MRI; 3 Tesla and higher) enabled its introduction to clinical practice. Today, tractography is an integral part of neurosurgical planning, enabling the identification and visualization of important neural pathways near pathological changes, such as gliomas or epileptic lesions. It also facilitates correlation with functional studies such as functional MRI (fMRI), transcranial magnetic stimulation (TMS), and intraoperative mapping of the cerebral cortex and nerve fibers (direct electrical stimulation [DES]) [3,4].
Among the different methods of white matter fiber reconstruction, two approaches – deterministic and probabilistic – are particularly evident. Deterministic tractography tracks a single trajectory based on the dominant diffusion direction in successive voxels. The method is fast and transparent, and its results are relatively easy to interpret. Probabilistic tractography, on the other hand, takes into account uncertainty in the direction of diffusion and generates probability distributions for many potential fiber pathways. Although it offers richer insight into complex anatomical structures, it requires more computational effort and its results are more difficult to interpret [5].
Deterministic tractography is considered to be more “clinically friendly” because it provides atlas-like representations of fiber pathways that are readily interpreted by neurosurgeons and facilitate their integration into intraoperative neuronavigation. However, this method is prone to errors in areas with low anisotropy (e.g. peritumoral edema) and at fiber intersections where a single tensor vector does not reflect actual anatomical complexity. Probabilistic tractography solves some of these problems, but generates results in the form of probability density maps that are not always intuitive to interpret and require experience [6-8].
This article is a narrative review aimed at providing a clinically oriented comparison of deterministic and probabilistic tractography. Given the heterogeneity of diffusion models, acquisition protocols, and validation methods across published studies, a systematic review or meta-analysis was not feasible.
Methods of tractography
Deterministic tractography
Deterministic tractography is based on the assumption that there is one dominant direction of diffusion in each voxel. The fiber course is determined step by step along the main vector of the diffusion tensor. This method, due to its simplicity, speed of calculation and ease of interpretation of results, is widely used in neurosurgical neuronavigation and in the analysis of large, well-organized white matter tracts, such as the cortical-spinal tract or the longitudinal upper bundle [9-11]. The algorithm tracks the trajectory of the fiber until the fractional anisotropy (FA) value drops below a set threshold or when the change of direction exceeds a specified angular limit (usually 35-60°). As a result, clear and unambiguous lines are obtained showing the course of nerve pathways [12,13].
The most important limitation of this method is its insufficient accuracy in the areas of intersections and fiber branches. Since the diffusion tensor model describes only one dominant direction, it does not allow for proper mapping of where the fibers intersect, touch, or branch. In such areas, the algorithm often terminates tracking prematurely, leading to false-negative results and a “loss” of some anatomically present tracts. This problem is particularly evident in the arcuate fasciculus (AF) region and in the temporal lobe, where the white matter architecture is extremely complex [10,14-16].
An additional limitation of deterministic tractography is its high sensitivity to pathological changes. Peritumoral edema, cancer infiltration or demyelination cause a decrease in FA values, which may result in interruption of tracking even in continuous nerve pathways. In practice, attempts are made to counteract this by modifying algorithm parameters such as lowering the FA threshold or reducing the maximum allowable steering angle, but this is associated with an increased risk of artefacts and incorrect reconstructions [17].
Probabilistic tractography
Probabilistic tractography was developed in response to the limitations of deterministic methods, especially in fiber reconstruction in areas with complex white matter architecture. Unlike the deterministic approach, which selects one dominant direction of diffusion in the voxel, probabilistic methods rely on probability distributions of diffusion directions. Instead of a single trajectory, multiple potential paths are generated, making it possible to take into account the measurement uncertainty due to the presence of noise, limited spatial resolution, and the coexistence of several fiber populations in a single voxel. The result of the analysis is a call density map, in which each voxel is assigned a value reflecting the probability of the course [18,19].
One of the main advantages of probabilistic tractography is its greater sensitivity in the imaging of complex structures. This method is particularly useful in the reconstruction of language routes, such as the AF or the frontal aslant tract (FAT), which are characterized by high individual variability and complicated anatomy. Research by Jenabi et al. [20] showed that the probabilistic approach allows for a fuller reproduction of these structures and more often indicates their continuity in areas covered by cancer infiltration or edema. Similarly, Zolal et al. [21] demonstrated the advantage of this method over deterministic tractography in cranial nerve imaging, while Schlaier et al. [22] confirmed its effectiveness in the reconstruction of cerebellothalamic connections.
The limitations of probabilistic tractography are mainly due to its greater complexity and high computational requirements. Generating thousands of possible trajectories involves longer analysis time and the need to use more efficient equipment compared to the deterministic method. In addition, interpretation of the results can be more difficult – unlike unambiguous streaming lines, probability density maps require experience and interpretive caution. In practice, it is necessary to set acceptance thresholds (e.g. 5-10% voxels with significant probability), which affect the final shape of the reconstruction and may introduce an element of subjectivity [9,10].
Despite these limitations, probabilistic tractography has found a permanent place in oncological neurosurgery and mapping of language functions, where the risk of fiber loss in deterministic reconstruction could lead to irreversible neurological deficits. In such cases, a probabilistic approach, often combined with fMRI and intraoperative DES, is now considered the standard of treatment [23]. This method is also used in deep brain stimulation (DBS) planning, where detailed knowledge of cerebellothalamic and limbic connections is crucial for predicting the effectiveness of treatment [24].
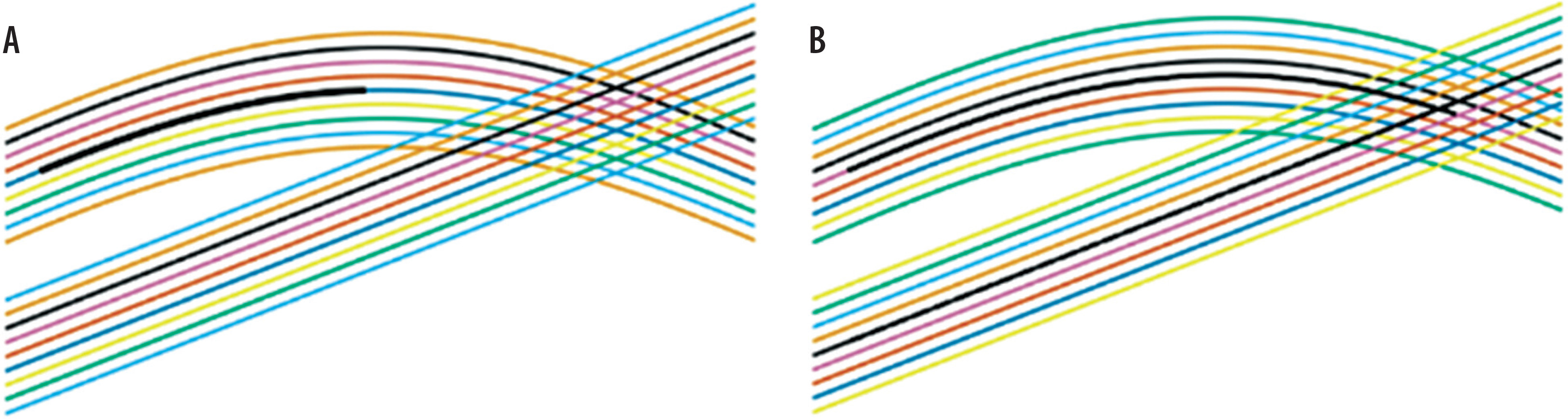
The diagram shown in Figure 1 w illustrates the principles of algorithms, not the actual results of the tractography. The ability to distinguish crossed fibers depends not only on the probabilistic model used, but also on the voxel model (e.g. constrained spherical deconvolution [CSD], high angular resolution diffusion imaging [HARDI]) and the angular resolution of the diffusion data.
Results
Comparison of deterministic and probabilistic tractography
Comparative studies indicate that deterministic tractography is particularly useful in imaging simple and well-isolated tracts, while probabilistic approaches show better effectiveness in areas with complex white matter fiber architecture [21]. Schlaier et al. [22] described the advantage of the probabilistic method in mapping cerebellothalamic connections, and Jenabi et al. [20] reported its high effectiveness in the reconstruction of language routes. Li et al. [25] stated that the probabilistic approach allows for a more accurate representation of the AF compared to the deterministic method.
A summary of the key features of both tractography algorithms is presented in Table 1.
Table 1
Comparison of deterministic and probabilistic tractography
[i] AF – arcuate fasciculus, CST – corticospinal tract, DBS – deep brain stimulation, DES – direct electrical stimulation, FA – fractional anisotropy, FAT – frontal aslant tract, fMRI – functional magnetic resonance imaging, nTMS – navigated transcranial magnetic stimulation, SLF – superior longitudinal fasciculus
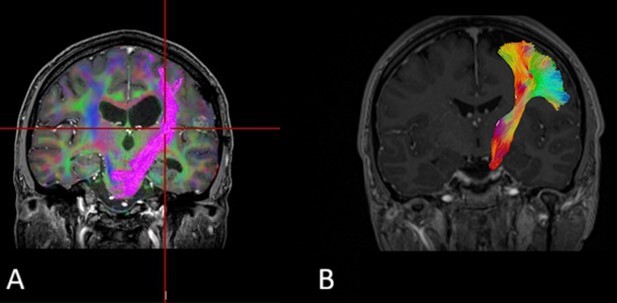
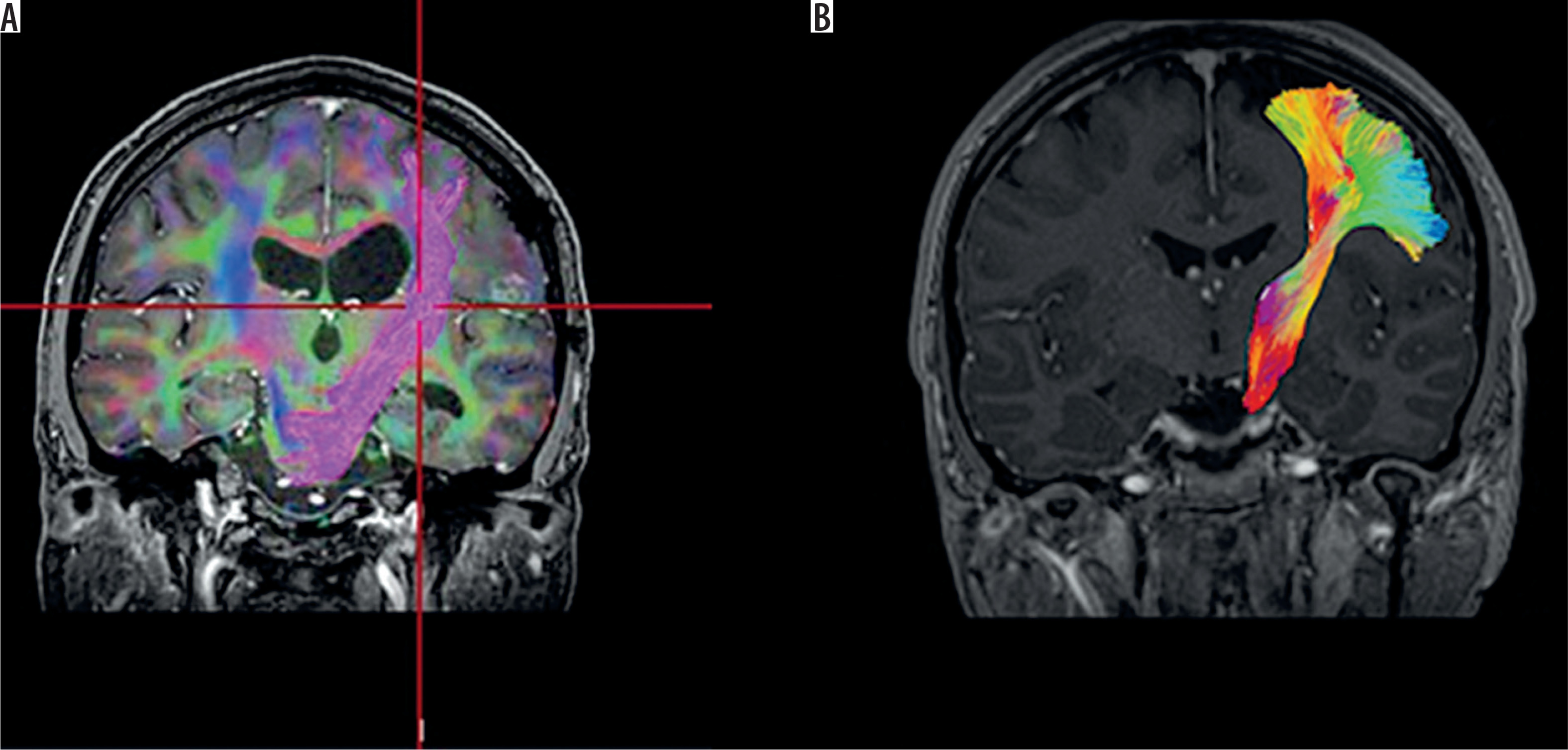
Figure 2 presents a comparison of the corticospinal tract reconstructed using deterministic (A) and probabilistic (B) tractography. The deterministic approach (A) generates clear, well-defined streamlines but may prematurely terminate in areas of fiber crossings, leading to incomplete visualization. In contrast, the probabilistic approach (B) produces a fuller and more continuous representation of the tract, offering greater sensitivity in regions with complex fiber architecture.
Figure 2
Comparison of corticospinal tract reconstructions using deterministic (A) and probabilistic (B) methods, displayed on the same anatomical background and color scale. The deterministic method yields clear but truncated streamlines, while the probabilistic reconstruction shows a denser and more continuous trajectory, especially near fiber crossings
Role of tractography in neuroradiological practice
Diffusion tensor imaging tractography is increasingly being used in neuroradiology as a complementary tool for the evaluation of brain MRI studies, particularly in cases where analysis of the spatial relationship of pathological changes to major white matter tracts is essential [24,26]. For neuroradiologists, tractography represents an extension of classical structural imaging, enabling a better understanding of the potential impact of pathology on the organization of white matter connections. However, it should be emphasized that the resulting reconstructions are model-based and do not directly reflect actual anatomy, requiring careful interpretation of the results [27,28].
In everyday diagnostic practice, deterministic tractography is most commonly used due to its relatively short reconstruction time, good image clarity, and ease of presentation in radiological documentation. This method is particularly effective in assessing large, well-organized white matter bundles, such as the corticospinal tract or optic radiation [14,29,30]. Its limitations become apparent in areas of fiber crossing, in regions with reduced FA, and in the presence of edema, where underestimation or fragmented visualization of neural tracts may occur [31,32].
In such cases, probabilistic tractography can be a valuable complement to neuroradiological analysis, enabling a more sensitive assessment of the complex architecture of white matter and potentially preserved connections that are not visible in deterministic reconstructions. This is particularly true for association tracts and areas with high interindividual variability. However, interpreting probabilistic density maps requires experience and the conscious selection of acceptance thresholds to avoid overinterpretation of results [33,34].
A crucial element of a neuroradiologist’s work is the proper reporting of tractography results. The examination description should clearly indicate the reconstruction method used and emphasize the dependence of the obtained results on the analysis parameters and the quality of the diffusion data. Tractography should be interpreted in correlation with structural imaging and clinical data, and its results should be considered a supportive, not definitive, element in the diagnostic process. The rational, complementary use of deterministic and probabilistic tractography increases the informative value of MRI examinations and contributes to the development of modern clinical neuroradiology [1,35,36].
Common interpretational challenges in clinical practice
Tractography should not be treated as a direct anatomical image, but rather as a mathematical model. Interpretation errors most often result from excessive confidence in the reconstruction, high sensitivity of the method to technical parameters (such as FA thresholds, step length or permissible curvature of fibers) and the omission of individual variability. Both deterministic and probabilistic trajectories require verification using functional methods such as DES, fMRI, and navigated TMS (nTMS) to ensure their clinical relevance [37].
The most common interpretive pitfalls include:
Overestimating the credibility of the image: Tractography is not an “anatomical map” in the literal sense of the term, but a model based on the distribution of water diffusion in tissue. Fiber lines should be considered as an approximation of the white matter trails, not their actual anatomical image [37,38].
Errors in the areas of intersections and fiber branches: In the deterministic method, reconstruction often ends prematurely, leading to the “disappearance” (false-negative results) of important nerve pathways. On the other hand, in the probabilistic approach, the volume of reconstruction may be excessive, resulting in the presence of false-positive fibers, especially in the absence of appropriate acceptance thresholds [39].
Effects of pathological changes: Swelling, tumor infiltration and demyelination cause a decrease in the value of FA and interfere with the continuity of fibers in reconstruction, even though a given pathway may be anatomically preserved. This may give the impression that the fiber has been permanently broken [40].
Dependence on technical parameters: Incorrect selection of FA thresholds, maximum deviation angle, or number of reconstruction steps can lead to significantly different results. Because data are often not standardized between study centers, comparison of studies can be difficult, and the same clinical case can be interpreted differently [25,40].
Overly literal use in neuronavigation: Tractographic images are often transferred to neuronavigational systems and treated as inviolable boundaries during tumor resection. It should be remembered, however, that they serve only an indicative function, and surgical decisions should be verified each time using functional methods, such as DES or nTMS [9,10].
Insufficient consideration of individual variability: Some pathways, especially those related to language function (e.g. AF), show significant variability between patients. As in other brain regions, comparing tractographic images with atlases can lead to erroneous conclusions [9].
Research results should be discussed in relation to previous publications and adopted working hypotheses, and their significance interpreted in the widest possible context. It is also advisable to take into account potential directions for further research.
Discussion
Clinical applications and development prospects
Beyond its clinical utility, tractography provides valuable insights into white matter organization for basic neuroscience. It supports the study of developmental myelination, interindividual variability in cortical connectivity, and structure–function coupling in networks underlying language, motor control, and cognition. Method developers employ tractography to test new diffusion models and to build population-based atlases, which help refine our understanding of the human connectome [41,42].
Tractography, both deterministic and probabilistic, is widely used in clinical practice. In neurosurgery for brain tumors, it enables the determination of the relationship of a pathological lesion to key tracts such as the corticospinal tract or the AF, allowing for resection planning with maximum preservation of motor and language functions [43]. In epilepsy surgery, it supports the identification of neural networks responsible for memory and cognitive functions. Furthermore, it facilitates a better understanding of the cerebellar-thalamic and limbic tracts in DBS planning, which ultimately translates into improved treatment effectiveness. In neurorehabilitation, tractography is used to assess the degree of post-stroke fiber damage and predict the recovery of motor and language functions [44,45].
The development prospects for tractography are related to the introduction of high-angle resolution techniques, such as HARDI and CSD, which allow for more accurate mapping of fiber crossing areas, as well as the integration of tractography with other imaging modalities, including fMRI, TMS, and intraoperative imaging (such as DES). Artificial intelligence (AI) will also become increasingly important, enabling automated region of interest selection and tract classification, as well as the creation of population atlases supporting personalized treatment. All of these development directions aim to make tractography not only an illustrative tool but, above all, a predictive and standardized one that supports clinical decisions in a repeatable and objective manner [37].
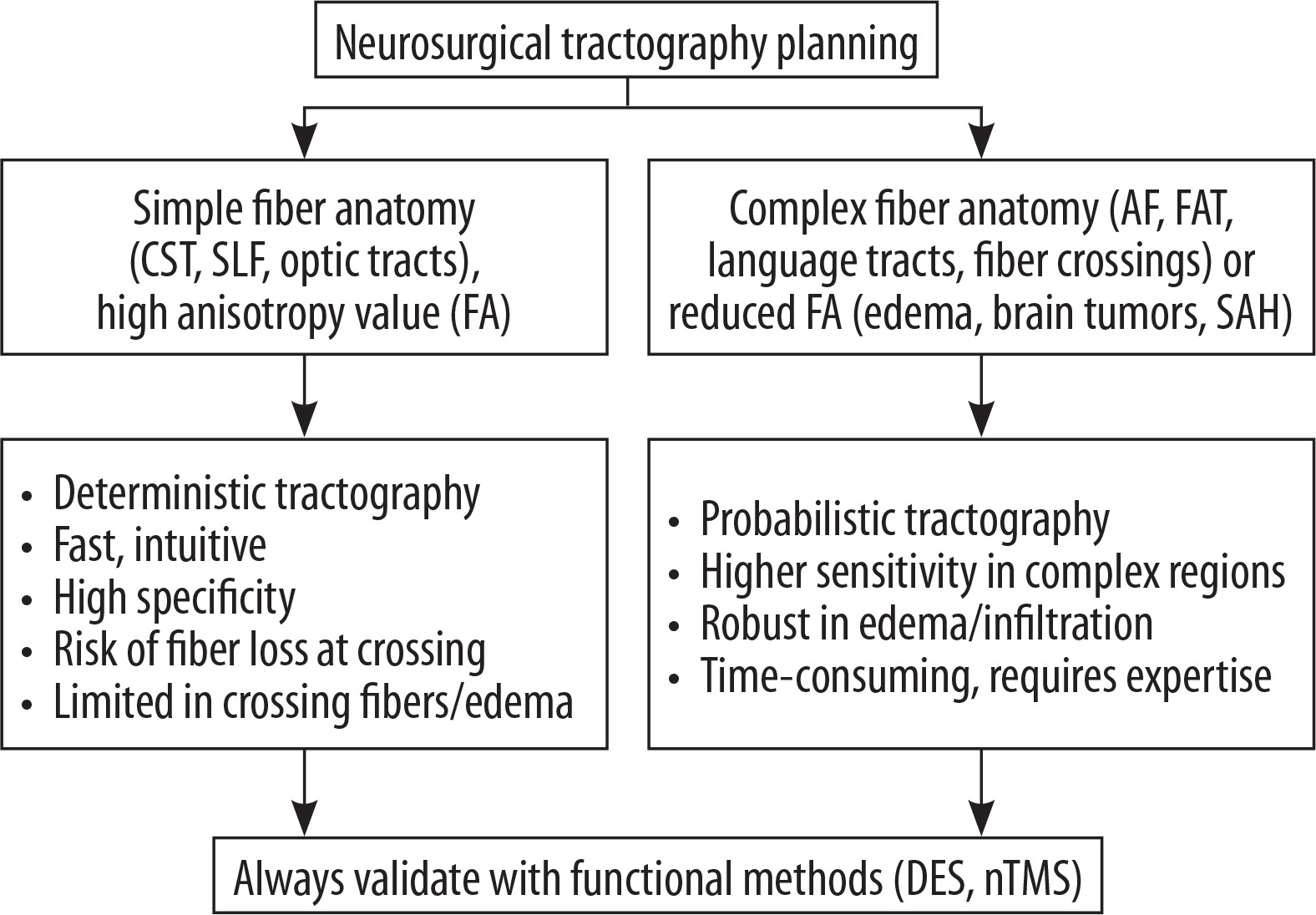
In parallel with technological progress, it is necessary to pay attention to the proper selection of the tractography method in neurosurgical planning. Deterministic algorithms are usually sufficient for large, well-organized bundles of fibers, such as the cortical-spinal route or the visual routes, where reconstruction is fast, intuitive and characterized by high specificity. However, their credibility decreases in areas with complex anatomy or reduced anisotropy, where fiber loss often occurs. In such situations, an advantage is offered by probabilistic tractography, which is characterized by greater sensitivity, especially within the linguistic tracts and in the areas of edema or tumor infiltration, although it is more time-consuming and requires more interpretative experience. Regardless of the method used, tractography results should always be cross-validated with functional mapping, such as DES or nTMS, in order to ensure clinical safety [9,23,24].
Decision-making algorithm for choosing deterministic or probabilistic tractography is presented in Figure 3.
Figure 3
Decision algorithm for neurosurgical tractography planning
AF – arcuate fasciculus, CST – corticospinal tract, DES – direct electrical stimulation, FA – fractional anisotropy, FAT – frontal aslant tract, nTMS – navigated transcranial magnetic stimulation, SLF – superior longitudinal fasciculus, SAH – subarachnoid hemorrhage
Role of artificial intelligence in tractography
The integration of HARDI, CSD, and AI-based reconstruction algorithms is significantly transforming tractography. Deep learning methods help reduce noise, generate fiber lines, and eliminate artefacts. AI also enables automatic classification of routes and integration of data from various modalities, such as fMRI and magnetoencephalography (MEG), which promises a shift from qualitative visualization to quantitative, standardized white matter network mapping. Artificial intelligence, and deep learning techniques in particular, promises significant advances in diffusion magnetic resonance imaging (dMRI) and tractography in the coming years [46]. AI is already being used in noise reduction, image quality improvement and more precise modelling of white matter microstructure, including noise reduction, artefact removal, resolution enhancement, and automatic quantification of dMRI parameters [36]. The most innovative approaches include fully generative end-to-end models, such as DDTracking, a diffusion-based method that models the propagation process of filaments (streaming lines) and outperforms classical tractography algorithms in terms of anatomical compatibility and overall reconstruction accuracy [47]. In a hybrid approach, the Bonn team developed a method combining traditional tractographic algorithms with AI, which allows the elimination of so-called “hallucinations” of tractions – i.e. the reconstruction of anatomically non-existent fibers – and increased precision of mapping, especially in pathological cases, such as post-hemispherotomy states [48].
Equally important is the development of data sets for training and validation of AI models. The newly developed Diff5T dataset provides raw data in k-space with images, allowing for more reliable and generalized multi-parameter reconstruction models in dMRI [49]. Other autoencoder-based approaches, such as filtering in tractography using autoencoders, have been designed to efficiently filter streaming lines by removing artefacts and inconsistent trajectories, significantly increasing the reliability of neural connectivity analyses [50].
Another promising development direction of tractography is the integration of AI with multimodal neurobiological imaging. Combining dMRI, fMRI, and electroencephalography or MEG data allows for more comprehensive models of neural networks in which AI supports automatic detection and correlation of functional structures with their anatomical counterparts [51]. This approach opens up the prospect of creating personalized brain maps that not only visualize the course of fibers, but also predict the functional consequences of potential surgical resections [52-54].
Conclusions
Deterministic and probabilistic tractography are complementary techniques that respond to different clinical needs. Deterministic methods are fast, intuitive and reliable in imaging large, well-defined tracts, while probabilistic approaches are more sensitive for complex fiber networks and are critical where the priority is to preserve neurological functions. Their combined use, especially in combination with functional mapping methods, increases the safety of surgical procedures and improves treatment outcomes. Future integration with advanced diffusion models and artificial intelligence will further enhance the accuracy, repeatability and clinical utility of tractography.