Introduction
The global burden of coronary artery disease (CAD) is increasing with the growth of aging populations and lifestyle risk factors such as diabetes, hypertension, smoking, and dyslipidemia, killing more than 9 million every year; it is the number one cause of death worldwide [1]. CAD is characterized by increased accumulation of atherosclerotic plaques in coronary arteries, leading to stenosis and ischemia and eventually myocardial infarction. Prompt detection of subclinical atherosclerosis and risk stratification are essential in managing guidelines for primary prevention and therapeutic intervention.
Classical CAD diagnostic methods include clinical risk scores, exercise treadmill testing (ETT), echocardiography, nuclear myocardial perfusion imaging (MPI), and invasive coronary angiography (ICA). Although ICA is considered the gold standard in anatomic assessment of coronary stenosis, it is confined to selected population groups due to being invasive, having complications, and high costs (Table 1). Noninvasive stress testing modalities, including ETT and MPI, show moderate sensitivity and specificity at best, especially in intermediate-risk populations.
Table 1
Comparison of traditional diagnostic tools and emerging imaging modalities in coronary artery disease evaluation
The capabilities of coronary angiogram imaging have been greatly enhanced with the advent of computed tomography angiography (CTA). Coronary artery vessels can now be visualized at high resolution with intra-cardiac nonobstructive plaques. In addition, CTA enables assessment of coronary plaque composition and quantification of calcified and non-calcified plaque burden [2]. Multicenter trials such as PROMISE and SCOT-HEART have successfully demonstrated the clinical utility of CTA in improving diagnostic certainty, in management of patients, and, potentially, long-term clinical outcomes [3,4].
Along with CTA, coronary artery calcium scoring (CACS) has attracted great attention as it helps in risk stratification and early detection of coronary atherosclerosis through non-contrast computed tomography (CT) imaging. CACS provides a quantitative measure known as the coronary artery calcium (CAC) score. CAC score measures the total coronary plaque burden using the Agatston score and is well correlated with cardiovascular events [5]. When the CAC score is equal to zero, it is regarded as a low risk of future cardiac events and is increasingly used as a “gatekeeper” in deferring further tests [6]. In contrast, a higher calcium scores significantly increase the risk of myocardial infarction and mortality [7,8].
Multiple meta-analyses have verified prognostic implications of CACS. Lo-Kioeng-Shioe et al. [2] demonstrated that elevated CAC significantly predicted major adverse cardiovascular events (MACE), while Sarwar et al. [9] confirmed the strong negative predictive value of zero calcium. Further evidence from various studies supports CACS and CTA as synergistic methods to improve diagnostic accuracy and stratify patients with suspected CAD.
Despite its importance as a prognostic tool, CACS has not found universal application in clinical practice because of variability in guidelines, concerns over cost-effectiveness, and radiation exposure. Nevertheless, with advancements in the field of CT technology and dose reduction techniques, the risk-benefit ratio is getting better for CACS. As evidence accumulates, major guidelines issued by the American College of Cardiology and the European Society of Cardiology increasingly recognize the use of calcium scoring for selected patient groups.
In keeping with the more fluid roles that CACS is assuming in today’s cardiovascular diagnostics, this systematic review and meta-analysis aims to comprehensively assess the diagnostic and prognostic performance of CACS in patients with suspected or known CAD. Specifically, the utility of CACS across different clinical presentations, populations, and in conjunction with CTA will be examined so that the current and possible future clinical application of CACS can be further elucidated.
Material and methods
Search strategy
This systematic review and meta-analysis was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Exhaustive literature searches were carried out on the databases of PubMed, Scopus, and Web of Science searching for any relevant study published from January 2008 to April 2024. The search terms consisted of combinations of “coronary artery calcium,” “CAC score,” “computed tomography,” “cardiac CT,” “CTA,” “coronary artery disease,” “diagnosis,” and “prognosis.” Boolean operators and Medical Subject Headings were used to narrow down the search.
Inclusion and exclusion criteria
Eligible studies met the following criteria:
original research articles published in English;
studies assessing the diagnostic or prognostic value of CACS in patients with suspected or known CAD;
use of CTA or non-contrast CT for CACS evaluation;
reporting of relevant outcomes such as diagnostic accuracy (sensitivity/specificity) or prognostic endpoints (major adverse cardiac events, all-cause mortality).
Exclusion criteria included:
Data extraction and synthesis
The two independent reviewers gathered lead data such as study design, population characteristics, imaging methods, CACS thresholds, and the outcome measures. Any discrepancy among them was resolved either by consensus or adjudication from a third party. In meta-analytic pooling, a random-effects model was used for merging sensitivity, specificity, and hazard ratios (HRs) to accommodate heterogeneity.
Quality assessment
Methodological quality assessment of the included studies was performed by applying the Quality Assessment of Diagnostic Accuracy Studies (QUADAS-2) tool for diagnostic studies and the Newcastle-Ottawa Scale (NOS) for prognostic ones. Both reviewers assessed bias risk, applicability, and validity of the study independently.
Results
Characteristics of included studies
A total of 14 studies were included in the qualitative analysis (Table 2), encompassing more than 81,743 participants across diverse geographic and demographic settings. The included populations comprised both symptomatic and asymptomatic individuals, patients with stable chest pain, diabetics, and those without a prior history of CAD. Most studies used non-contrast cardiac CT for CACS, while a subset incorporated both CACS and coronary CTA. Follow-up durations for prognostic assessment ranged from 2 to 10 years. The Agatston scoring system was consistently applied across studies, using standard categories: CAC = 0 (no calcification), CAC 1-99 (mild), CAC 100-399 (moderate), and CAC ≥ 400 (severe).
Table 2
Characteristics of included studies
| Author/year | Country | Sample size | Population type | Imaging method | Follow-up period | Outcomes measured |
|---|---|---|---|---|---|---|
| Chaikriangkrai et al., 2016 [1] | USA | 3,063 | Symptomatic | CACS + CTA | 3 years | MACE, all-cause mortality |
| Lo-Kioeng-Shioe et al., 2020 [2] | Multi-national | 34,000 | Symptomatic | CACS | 5 years | MACE, CAD-related mortality |
| Koopman et al., 2022 [3] | Netherlands | 1,200 | Stable chest pain | CACS + CTA | 2 years | Obstructive CAD, hospitalization |
| Tramontano et al., 2022 [4] | Italy | 5,216 | Asymptomatic | CACS | 4.5 years | Cardiovascular events, death |
| Sarwar et al., 2009 [9] | USA | 27,125 | Mixed (symptomatic + asymptomatic) | CACS | 5 years | Prognosis with CAC = 0 |
| den Dekker et al., 2012 [10] | Netherlands | 1,408 | Symptomatic | CTA stratified by CACS | 3 years | Diagnostic accuracy based on CAC levels |
| Kramer et al., 2013 [11] | Canada | 6,521 | Diabetic patients | CACS | 5 years | All-cause mortality, cardiovascular events |
| Agha et al., 2022 [12] | USA | 3,210 | Chest pain (low-risk) | CACS | 2-4 years | Prognostic value of CAC = 0 |
Diagnostic value
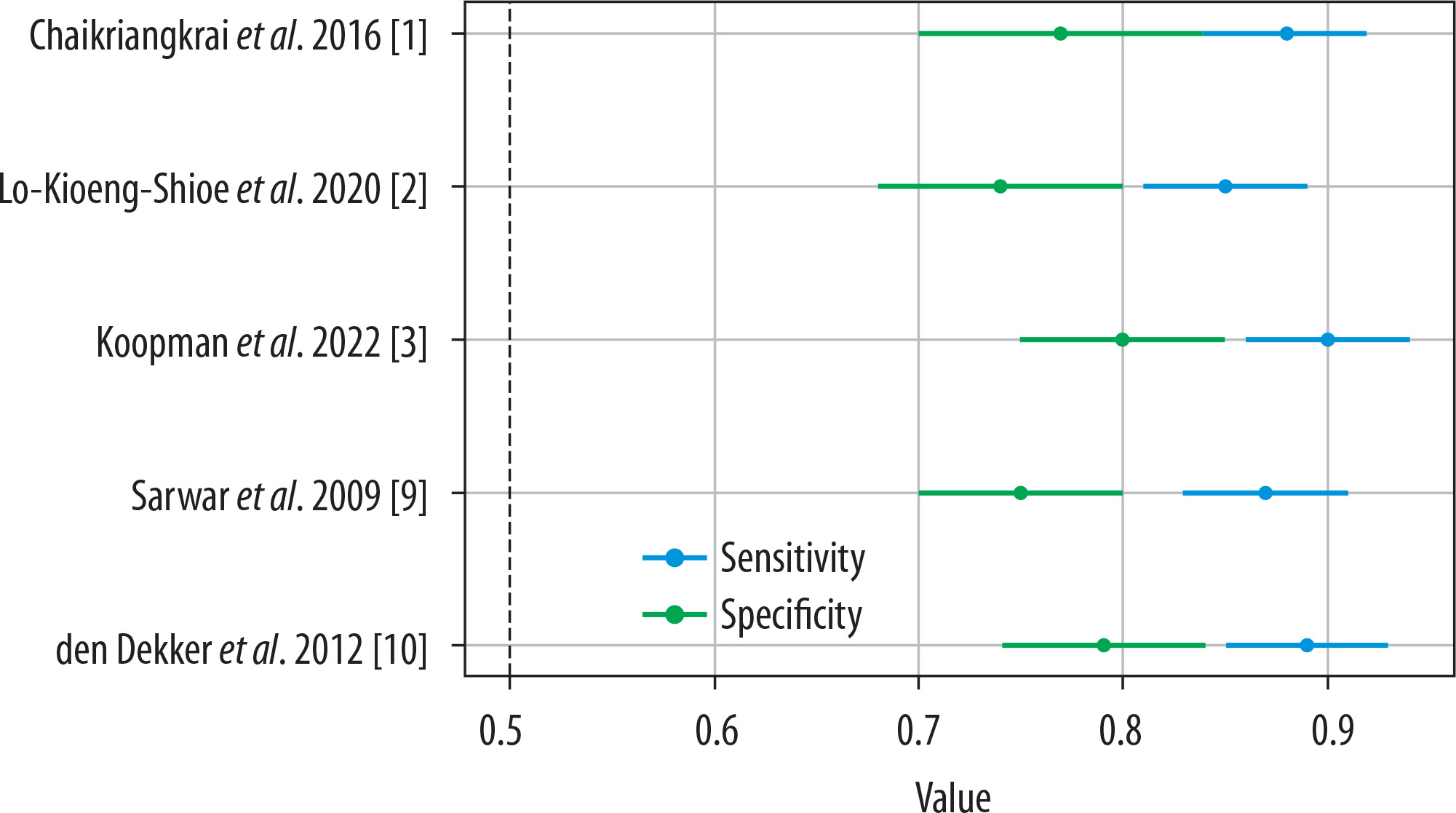
Among patients in low-to-intermediate risk categories, the addition of CACS significantly enhanced the diagnostic performance of CTA. The pooled sensitivity for detecting obstructive CAD (≥ 50% stenosis) was 88% (95% confidence interval [CI]: 84-91%) and pooled specificity was 77% (95% CI: 70-83%) when CACS was combined with CTA (Figure 1) [9,10]. The presence of any coronary calcification (CAC > 0) showed a strong association with obstructive CAD. However, the diagnostic accuracy of CTA was reduced in patients with very high calcium scores (CAC ≥ 400) due to blooming artifacts, which may obscure luminal visualization.
Prognostic value
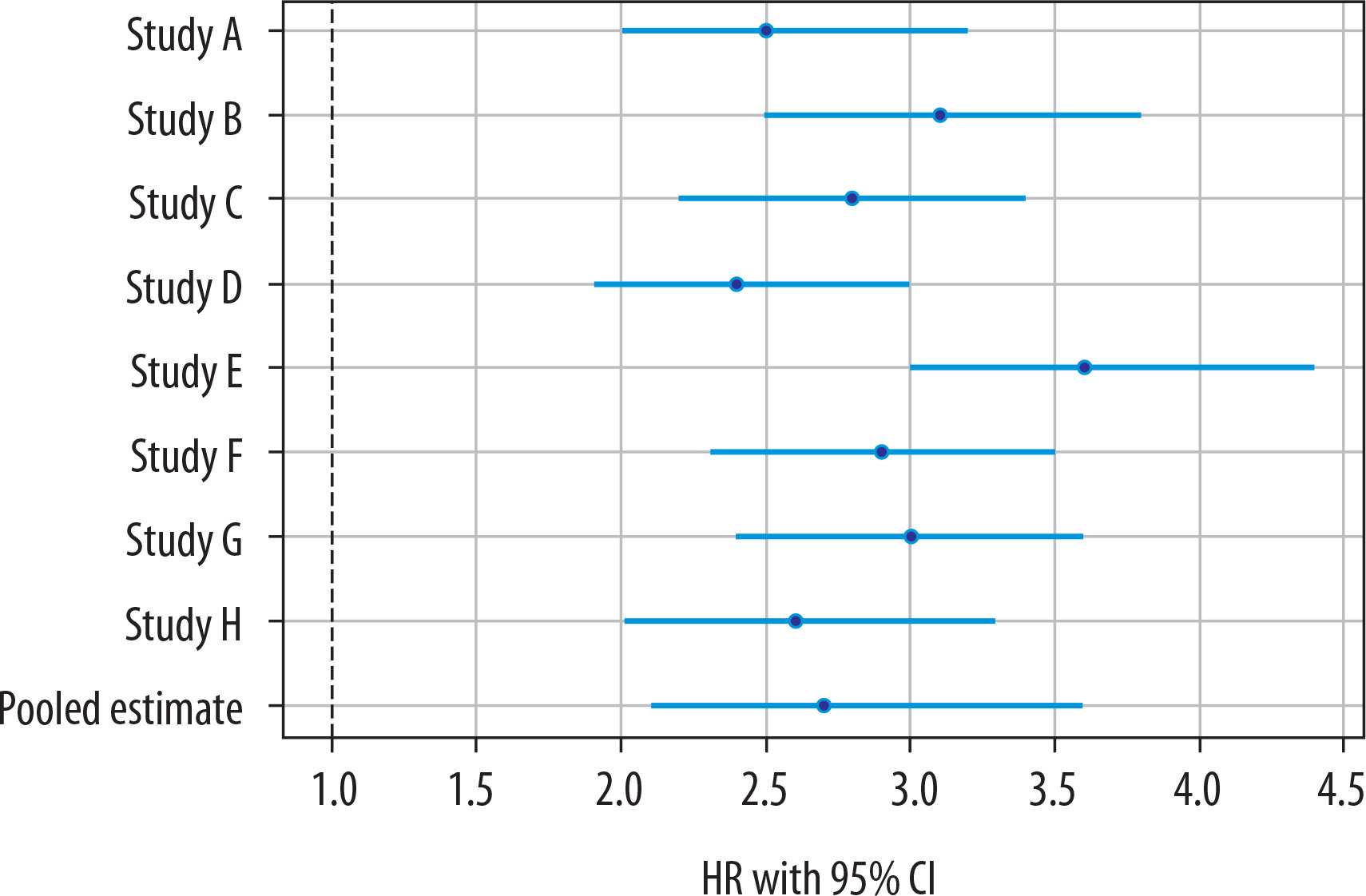
Elevated CAC scores were consistently associated with increased risk of MACE. Patients with CAC ≥ 100 demonstrated a pooled HR of 2.7 (95% CI: 2.1-3.6) for future cardiac events compared with individuals with CAC = 0 (Figure 2) [11]. Conversely, a CAC score of zero was strongly associated with an excellent prognosis, with event rates remaining below 1% over a 5-year follow-up period [9,12].
Subgroup analyses
In asymptomatic individuals, a CACS of zero demonstrated a high negative predictive value for cardiac events [7]. However, even mild calcification (CAC 1-99) was associated with an increased risk of cardiac events in diabetic patients compared to non-diabetic individuals with similar scores [8,13]. The prognostic utility of CACS remained consistent across different age groups, sexes, and ethnic populations, although higher scores were more frequently observed in older individuals and males [10].
Discussion
This systematic review and meta-analysis further confirms that CACS provides significant diagnostic and prognostic value in the assessment of CAD. The findings consistently demonstrate that CACS, particularly when combined with coronary CTA, enhances early diagnosis and risk stratification across diverse populations, including asymptomatic individuals, diabetics, and patients with stable chest pain.
One of the most important findings of this study is that higher CAC scores are strong predictors of MACE. Patients with a CAC score ≥ 100 exhibited nearly a threefold increased risk of future cardiac events compared to those with a CAC score of zero [11]. These findings reinforce the role of CACS as a robust long-term prognostic marker and highlight its importance in guiding preventive strategies.
Equally significant is the prognostic implication of a CAC score of zero. The absence of coronary calcification is consistently associated with excellent clinical outcomes and very low event rates over intermediate follow-up periods [9,12]. This supports the concept of the “power of zero,” which has important clinical implications in safely deferring further diagnostic testing or aggressive therapeutic interventions in low- to intermediate-risk patients.
Despite its advantages, certain limitations of CACS must be considered. In patients with extensive calcification (CAC score ≥ 400), the diagnostic performance of CTA may be compromised due to blooming artifacts, which can obscure luminal visualization and reduce specificity, potentially leading to false-positive findings [10]. However, while high calcium scores indicate elevated risk, they may simultaneously limit accurate anatomical assessment.
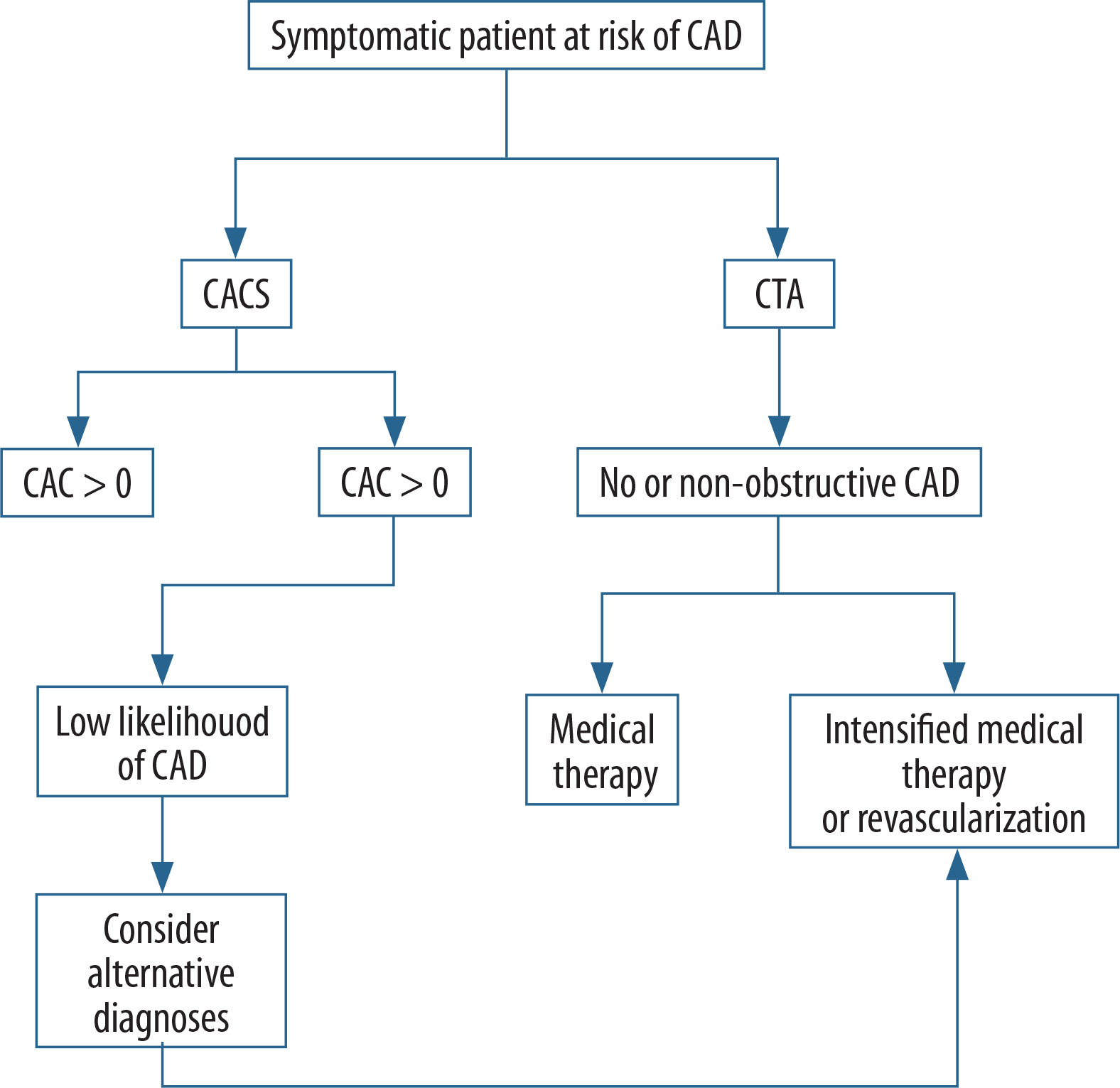
The combined use of CACS and CTA provides complementary information, improving overall clinical decision-making. While CACS reflects total plaque burden, CTA allows detailed evaluation of plaque composition and luminal stenosis. Discrepancies between the two modalities have been reported, such as high CAC scores with low Coronary Artery Disease – Reporting and Data System (CAD-RADS) scores due to masking effects of calcification, or low/zero CAC scores with high CAD-RADS scores in cases of non-calcified plaques. These observations highlight the importance of integrating both modalities for comprehensive cardiovascular assessment (Figure 3).
Figure 3
Integration of coronary artery calcium scoring (CACS) and coronary computed tomography angiography (CTA) in clinical decision-making for coronary artery disease (CAD)
CAC – coronary artery calcium
CACS also demonstrates consistent applicability across specific subgroups. In diabetic patients, even low levels of coronary calcification are associated with a significantly higher risk of cardiac events compared to non-diabetic individuals [8,13]. Furthermore, although calcium score distributions vary with age, sex, and ethnicity, its predictive value remains robust across different populations [10].
Despite the strengths of this meta-analysis, including a large pooled sample size and comprehensive evaluation of both diagnostic and prognostic outcomes, certain limitations should be acknowledged. Heterogeneity in study design, population characteristics, follow-up duration, and outcome definitions may introduce variability in the results. Additionally, not all included studies fully adjusted for conventional cardiovascular risk factors, which may act as confounders.
In conclusion, CACS is a reliable, non-invasive tool for both diagnosis and prognosis of CAD. Its integration with CTA enhances risk stratification and supports more precise, patient-specific clinical decision-making, reinforcing its role in contemporary cardiovascular imaging.
Conclusions
Our systematic review and meta-analysis highlights the significance of coronary calcium scoring as a non-invasive, cost-effective, and clinically useful tool for diagnosis and prognosis of CAD. CACS has been observed to be a highly predictive marker of MACE in a broad range of populations, particularly when its values exceed 100. CACS can also be used together with CTA to enhance the diagnostic accuracy of obstructive versus non-obstructive CAD, especially in low- to intermediate-risk patients.
One clinically significant finding is that a CAC score of zero is a reliable predictor of a very low risk of cardiovascular events in the short to intermediate term. This finding is increasingly being accepted to support the use of CACS as a gatekeeper to avoid exposing asymptomatic or low-risk persons to unnecessary invasive testing. Conversely, high CAC scores not only predict negative results but may demonstrate the potential failings of CTA interpretation because of blooming artifacts.
There is also evidence supporting the use of CACS in some high-risk subgroups including diabetics where even low calcium scores put the patient in a higher risk category. These insights may be used in clinical practice to personalize the risk stratification, guide therapeutic decision making, and streamline imaging resources.
In conclusion, CACS represents a central component of contemporary cardiovascular imaging protocols. The next phase of investigations should focus on establishing standard cutoff values, population-based risk profiles, and long-term outcome validation to further support the implementation of CACS in global CAD management.