Introduction
Breast cancer is one of the most common and prevalent malignancies affecting women worldwide. As per a recent study based on the latest statistics of GLOBOCAN (2022), the incidence of breast cancer is reported to be 11.6% in the world [1] and 13.8% in India [2]. Timely and accurate diagnosis of breast cancer is important because it helps reduce morbidity and mortality [3]. An essential diagnostic tool for breast lesions is ultrasonography (US), which is one of the most convenient and the cheapest all-time non-radiating investigations, which classifies the breast lesions through BI-RADS (Breast Imaging Reporting and Data System) classification [4].
Radiological imaging and diagnosis have become important because of the variable incidence of breast cancer, with most of the masses being benign in nature and calling for unnecessary biopsies [5].
Although conventional grey scale US and mammography remain standard investigations of imaging for breast lesions, contrast-enhanced ultrasound (CEUS) has become evident as a better tool for distinguishing malignant from benign breast masses [6,7]. The characteristic microbubble contrast agents, which are used in CEUS, show enhancement for a solid mass with higher vascular flow, indicating angiogenesis characteristically pointing towards malignant breast lesions, helping to differentiate from benign lesions [8,9]. Its applications have been consistently used also in liver lesions, and evidence continues to grow also for breast lesions.
CEUS had shown varied sensitivity of 64% to 89.4% and specificity of 66.4% to 89.74% [10-12] for differentiating between benign and malignant lesions and the quantitative parameter with high diagnostic purpose remains variable in terms of enhancement in vascularity [13,14].
Not many Indian studies have been conducted to determine the diagnostic accuracy of CEUS in differentiating benign and malignant lesions. Thus, the present study was carried out to study the diagnostic role of CEUS in terms of sensitivity, specificity, and its comparison with conventional grey-scale US with colour Doppler. The secondary objective was to assess the association of various CEUS parameters with benign and malignant breast lesions. The results of the study may allow for better diagnosis and management of the patients.
Material and methods
An observational study was performed for a duration of 18 months, i.e. from June 2023 to December 2024, whereby patients were enrolled. Inclusion criteria were adult females with breast masses detected clinically or incidentally and confirmed on conventional US. Exclusion criteria were patients with ongoing treatment or intervention for breast masses; masses being diagnosed as simple cysts or aberrations in normal development and involution (ANDI) on radiological examination; and pregnancy.
Sample size
The sample size was based on the study by Luo et al. [6], who observed that the sensitivity and specificity of CEUS for predicting malignancy was 85.4% and 87.8%, respectively. Taking these values as reference, the minimum required sample size with desired precision of 20%, 80% power of the study, and 5% level of significance was 57 patients (30 + 27). To reduce the margin of error, the total sample size taken was 64.
After enrolling, all patients were examined clinically by an experienced surgeon as per the standard guidelines. The age of the patients was noted. Patients underwent various investigations in the form of conventional US with colour Doppler and CEUS.
Grey-scale US: In each patient, breast US was performed in both the transverse and longitudinal planes using a Siemens Acuson S3000 US scanner with a linear-array transducer of frequency 4-9 Mhz.
Colour Doppler was performed in Colour Doppler, Power Doppler, and Spectral Doppler modes, using a linear array transducer of frequency 4-9 Mhz on a Siemens Acuson 3000 US Scanner. The number of vessels within the breast mass, pattern of vascularity (central/circumferential/penetrating vessel), presence of bidirectional arterial blood flow, peak systolic velocity, resistive index, and pulsatility index were documented, and data were saved digitally for data analysis [6]. Colour Doppler was used as an adjunct modality to grey-cale US in diagnosing breast masses. BI-RADS criteria for US were used to classify each lesion detected on US.
CEUS was performed using a linear array transducer of frequency 4-9 MHz on a Siemens Acuson S3000 US scanner with low mechanical index settings. After injecting 2.4 ml of intravenous contrast Sonovue (sulphur hexafluoride) followed by flushing with 10 ml of normal saline, the linear probe was kept on the breast mass for 6 min. Qualitative enhancement parameters like enhancement degree, internal homogeneity, perfusion defect, enhancement order, enhancement margin, and radial or penetrating vessel were assessed. A region of interest (ROI) was defined, encompassing most of the mass with sufficient area of normal tissue. An ROI curve was plotted, and quantitative parameters like mean transit time, time to peak, peak intensity, and area under time intensity curve were documented using Contrast Dynamics software.
Follow up and outcomes
US-guided fine needle aspiration cytology was done for all patients under complete aseptic precautions. In cases where the cytology result was equivocal, US-guided biopsy was done. Patients underwent surgery, and histopathological examination was done on the surgical specimen for confirmation of benign or malignant lesion.
Patients were followed-up in the hospital where they underwent surgery, and the surgical specimen was sent to the histopathological lab for histopathological examination by H&E and confirmation of benign or malignant lesion.
BI-RADS classification was given [15]. Outcome measures were the proportion of benign and malignant lesions of the breast and the diagnostic accuracy of CEUS to characterise malignant lesions in the breast.
Statistical analysis
Statistical analysis was performed using appropriate descriptive and inferential methods. Categorical variables were presented as frequencies and percentages, whereas continuous variables were summarised as mean ± standard deviation for normally distributed data and as median with interquartile range (25th-75th percentiles) for non-normally distributed data. Normality was assessed using the Shapiro-Wilk test. Group comparisons for continuous variables were conducted using the independent t-test or Mann-Whitney U test, as applicable. Associations between categorical variables were analysed using the c2 test, with Fisher’s exact test employed when expected cell counts were < 5. Diagnostic accuracy of B-mode US with colour Doppler and CEUS was evaluated by calculating sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV), using histopathological diagnosis as the reference standard. Agreement between radiological findings and histopathology was assessed using Cohen’s κ statistic. Data were entered in Microsoft Excel and analysed using SPSS software (IBM Corp., Chicago, USA; version 25.0), and a p-value < 0.05 was considered statistically significant.
Results
The mean age of study subjects was 41.16 ± 9.2 years. Among study subjects, 36 (56.25%) had lesions on the right side, and 28 (43.75%) had them on the left. Shape was irregular in 34 (53.13%) subjects, oval in 19 (29.69%), round in 9 (14.06%), and regular in 2 (3.13%). Margins were uncircumscribed in 37 (57.81%) cases and circumscribed in 27 (42.19%). A BI-RADS score of 5 was seen in 36 (56.25%) cases, 3 in 17 (26.56%), and 4 in 11 (17.19%). The mean value of USG length and breadth of breast masses were 3.42 ± 1.61 cm and 2.63 ± 1.23 cm, respectively (Table 1).
Table 1
Distribution of clinical characteristics
Among the patients, 51 (79.69%) showed the presence of vascularity on colour Doppler, while 13 (20.31%) had no vascularity.
CEUS findings showed that 42 (65.63%) patients had heterogeneous internal homogeneity, while 22 (34.38%) had homogeneous internal homogeneity. Enhancement order was centripetal in 35 (54.69%) cases, centrifugal in 20 (31.25%), and diffuse in 9 (14.06%). An irregular enhancement margin was observed in 36 (56.25%) cases, whereas 28 (43.75%) had a regular margin. Perfusion defects were identified in 31 (48.44%) cases and were absent in 33 (51.56%) cases (Table 2).
Table 2
Findings on contrast-enhanced ultrasound (CEUS)
Histopathological diagnosis revealed malignancy in 38 (59.38%) cases and benign pathology in 26 (40.63%) cases.
Among histopathological types identified, invasive ductal carcinoma was the most common, accounting for 36 (56.25%) of all cases. This was followed by fibroadenoma, which constituted 22 (34.38%) cases. Less common findings included phyllodes tumour in 4 (4.69%) cases, intraductal papilloma in 1 (1.56%), papillary lesion in 1 (1.56%), and hamartoma in 1 (1.56%) case.
The mean ± SD value of resistance index (RI) was 0.89 ± 0.36, pulsation index (PI) was 1.78 ± 0.95, peak systolic blood flow velocity (PSV) was 20.02 ± 11.83, mean transit time (MTT) was 46.55 ± 45.65, and time to peak (TTP) was 29.44 ± 30.88.
While comparing characteristics between benign and malignant lesions, malignant breast lesions exhibited distinct imaging characteristics compared to benign ones. Although the side of involvement (right vs. left) was comparable between groups, malignant cases showed significantly higher proportions of BI-RADS 5 categorisation, irregular shape, uncircumscribed margins, and Doppler vascularity (p < 0.0001). Malignant lesions more frequently demonstrated heterogeneous echotexture, perfusion defects, centripetal enhancement patterns, irregular enhancement margins, and radial or penetrating vessels. While age, lesion size, RI, PSV, MTT, and TTP did not differ significantly, perfusion-related parameters – PI, perfusion index values, and area under the curve (AUC) – were significantly elevated in malignant lesions (p < 0.01) (Table 3).
Table 3
Association of parameters with histopathological diagnosis
| Parameters | Benign | Malignant | Total | p-value |
|---|---|---|---|---|
| Site | ||||
| Left | 12 (46.15%) | 16 (42.11%) | 28 (43.75%) | 0.748† |
| Right | 14 (53.85%) | 22 (57.89%) | 36 (56.25%) | |
| BI-RADS | ||||
| 3 | 14 (53.85%) | 3 (7.89%) | 17 (26.56%) | < 0.0001* |
| 4 | 10 (38.46%) | 1 (2.63%) | 11 (17.19%) | |
| 5 | 2 (7.69%) | 34 (89.47%) | 36 (56.25%) | |
| Shape | ||||
| Regular | 1 (3.85%) | 1 (2.63%) | 2 (3.13%) | < 0.0001* |
| Round | 7 (26.92%) | 2 (5.26%) | 9 (14.06%) | |
| Oval | 17 (65.38%) | 2 (5.26%) | 19 (29.69%) | |
| Irregular | 1 (3.85%) | 33 (86.84%) | 34 (53.13%) | |
| Margins | ||||
| Uncircumscribed | 4 (15.38%) | 33 (86.84%) | 37 (57.81%) | < 0.0001* |
| Circumscribed | 22 (84.62%) | 5 (13.16%) | 27 (42.19%) | |
| Pattern of vascularity | ||||
| Absent | 12 (46.15%) | 1 (2.63%) | 13 (20.31%) | < 0.0001* |
| Present | 14 (53.85%) | 37 (97.37%) | 51 (79.69%) | |
| Enhancement degree | ||||
| Hyper | 7 (26.92%) | 36 (94.74%) | 43 (67.19%) | < 0.0001* |
| Hypo | 19 (73.08%) | 1 (2.63%) | 20 (31.25%) | |
| Iso | 0 (0%) | 1 (2.63%) | 1 (1.56%) | |
| Internal homogeneity | ||||
| Heterogeneous | 4 (15.38%) | 38 (100%) | 42 (65.63%) | < 0.0001* |
| Homogeneous | 22 (84.62%) | 0 (0%) | 22 (34.38%) | |
| Perfusion defects | ||||
| Absent | 25 (96.15%) | 8 (21.05%) | 33 (51.56%) | < 0.0001* |
| Present | 1 (3.85%) | 30 (78.95%) | 31 (48.44%) | |
| Enhancement order | ||||
| Centrifugal | 17 (65.38%) | 3 (7.89%) | 20 (31.25%) | < 0.0001* |
| Centripetal | 1 (3.85%) | 34 (89.47%) | 35 (54.69%) | |
| Diffuse | 8 (30.77%) | 1 (2.63%) | 9 (14.06%) | |
| Enhancement margin | ||||
| Regular | 25 (96.15%) | 3 (7.89%) | 28 (43.75%) | < 0.0001* |
| Irregular | 1 (3.85%) | 35 (92.11%) | 36 (56.25%) | |
| Radial or penetrating vessel | ||||
| Absent | 26 (100%) | 22 (57.89%) | 48 (75%) | < 0.0001* |
| Present | 0 (0%) | 16 (42.11%) | 16 (25%) | |
| Diagnosis B mode | ||||
| Benign | 22 (84.62%) | 3 (7.89%) | 25 (39.06%) | < 0.0001* |
| Malignant | 4 (15.38%) | 35 (92.11%) | 39 (60.94%) | |
| Diagnosis B mode + colour Doppler | ||||
| Benign | 22 (84.62%) | 3 (7.89%) | 25 (39.06%) | < 0.0001* |
| Malignant | 4 (15.38%) | 35 (92.11%) | 39 (60.94%) | |
| Diagnosis CEUS | ||||
| Benign | 25 (96.15%) | 0 (0%) | 25 (39.06%) | <.0001* |
| Malignant | 1 (3.85%) | 38 (100%) | 39 (60.94%) | |
| Age (years) | 38.58 ± 9.84 | 42.92 ± 8.47 | 41.16 ± 9.23 | 0.064‡ |
| USG length | 3.1 (2.025-3.662) | 3.4 (2.5-4) | 3.3 (2.3-4) | 0.167§ |
| USG breadth | 2 (1.6-3.662) | 2.3 (1.825-3.475) | 2.25 (1.775-3.525) | 0.345§ |
| RI | 0.7 (0.61-0.84) | 0.9 (0.78-1.1) | 0.86 (0.7-1.075) | 0.059§ |
| PI | 1.3 (0.8-1.7) | 1.9 (1.5-2.1) | 1.8 (1.3-2.1) | 0.006§ |
| PSV | 18 (12-23) | 21 (9.5-33) | 19.5 (9.6-32.5) | 0.707§ |
| MTT | 33 (23.75-54) | 33.5 (23-45) | 33.5 (23-52.25) | 0.642§ |
| TTP | 24.5 (15.25-33.5) | 21 (13.25-29) | 23 (14-30.5) | 0.301§ |
| PI | 40 (31.25-45) | 63.5 (47.75-69.5) | 53.5 (34.75-67.25) | 0.001§ |
| AUC | 360 (325-764) | 1200 (925-2000) | 1000 (410-1400) | < 0.0001§ |
On κ analysis, good agreement was found between histopathological diagnosis and diagnosis B mode + colour Doppler with κ 0.772 and p-value < 0.0001. Among 26 patients diagnosed as benign via histopathological diagnosis, 22 patients had similar findings in diagnosis B mode + colour Doppler. Among 38 patients diagnosed as malignant via histopathological diagnosis, 35 patients had similar findings in diagnosis B mode + colour Doppler. Othe overall concordance rate was 89.06%, and the overall discordance rate was 10.94% between histopathological diagnosis and Diagnosis B mode + colour Doppler.
On the other hand, CEUS showed very good agreement with histopathological diagnosis, with κ = 0.967 and p-value < 0.0001. Among 26 patients diagnosed as benign via histopathological diagnosis, 25 patients had similar findings in diagnosis by CEUS. Among 38 patients diagnosed as malignant via histopathological diagnosis, all patients had similar findings in diagnosis by CEUS. The overall concordance rate was 98.44%, and the overall discordance rate was 1.56% between histopathological diagnosis and CEUS (Table 4).
Table 4
Inter-rater κ agreement between histopathological diagnosis and diagnosis B mode + colour Doppler and diagnosis contrast-enhanced ultrasound (CEUS)
CEUS demonstrated sensitivity of 100% (95% CI: 90.75% to 100.00%), specificity of 96.15% (95% CI: 80.36% to 99.90%), and AUC of 0.98. It also achieved a PPV of 97.44% and NPV of 100%, with overall diagnostic accuracy of 98.44%. In comparison, Diagnosis B mode + colour Doppler yielded a sensitivity of 92.11%, specificity of 84.62%, PPV of 89.74%, NPV of 88.00%, and diagnostic accuracy of 89.06%, with an AUC of 0.88 (Table 5).
Table 5
Sensitivity, specificity, PPV, and NPV of diagnosis B mode + colour Doppler and diagnosis contrast-enhanced ultrasound (CEUS) for predicting malignancy
Representative case images are shown in Figures 1-5.
Figure 1
A-F shows grey scale ultrasound (US), colour Doppler, contrast-enhanced ultrasound (CEUS) study, and histopathology image of a 48-year-old female (patient no. 24), who presented with hard lump in her left breast. Grey-scale US (A, B) shows a heterogeneously hypoechoic mass with speculated margins in 3 to 5 o’clock position on the left breast. Colour Doppler (C) shows internal vascularity within the mass lesion. CEUS (C) shows heterogenous enhancement with perfusion defects (red arrow) and centripetal (order of) enhancement with radial vessels (yellow arrow). Quantitative CEUS (E) shows PI 65%, TTP 27 s, AUC 2300 s, and MTT 34 s. The grey-scale ultrasound, colour Doppler, and CEUS features were suggestive of malignant lesion. Histopathology (F) confirmed the features of invasive ductal carcinoma, with infiltrating and pleomorphic tumour cells forming tubules
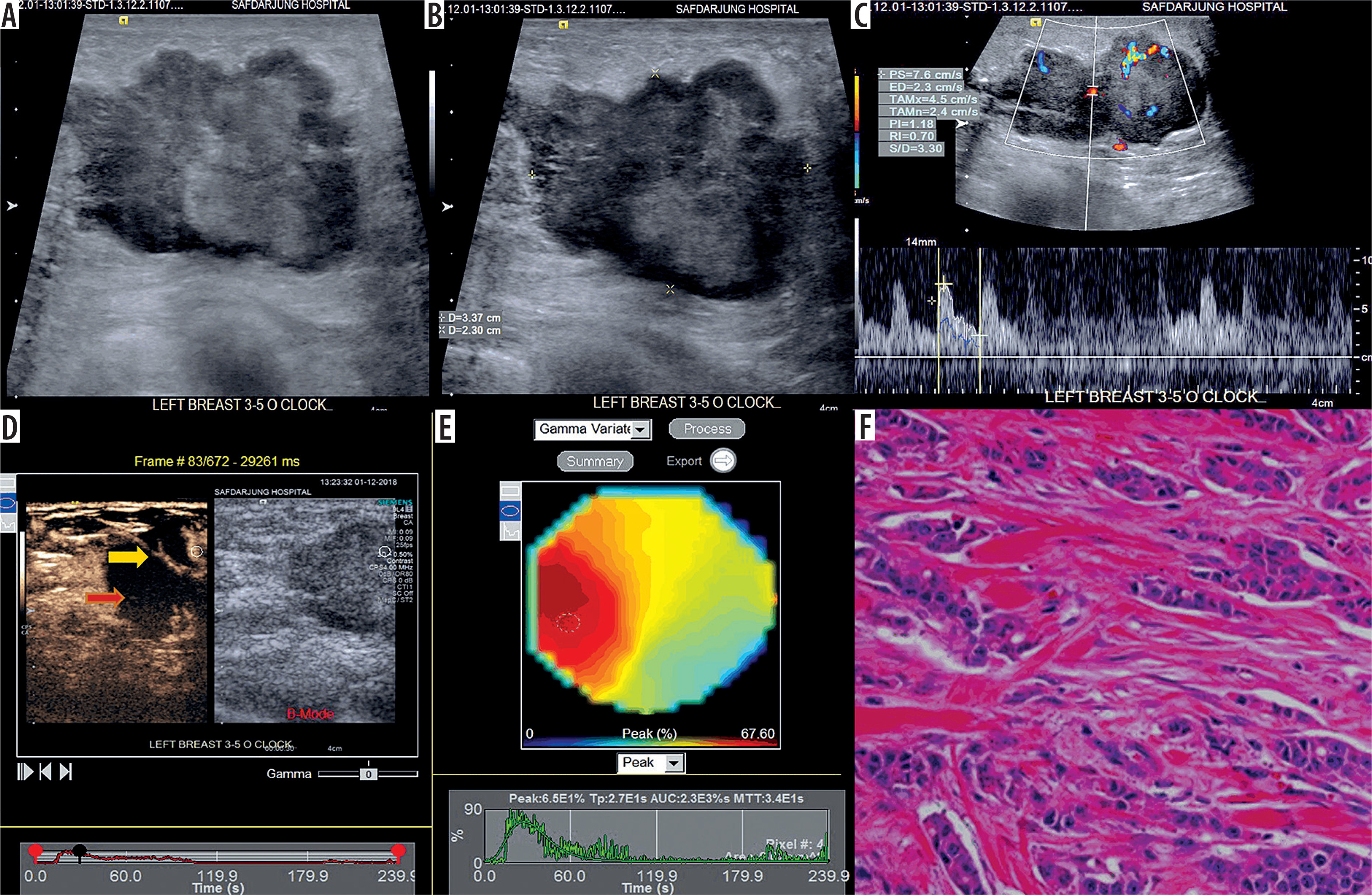
Figure 2
A-F shows grey-scale ultrasound (US), colour Doppler, contrast-enhanced ultrasound (CEUS), and histopathology image of a 45-year-old female who presented with hard lump in her left breast. Grey-scale US (A, B) shows a irregular, heterogeneously hypoechoic mass with uncircumscribed margins with few calcific foci in 12 to 3 o’clock position on the right breast. Colour Doppler (C) shows internal vascularity within the mass lesion. CEUS (E) shows heterogenous enhancement with multiple large perfusion defects (red arrow) and centripetal (order of) enhancement. Quantitative CEUS (E) shows PI 53%, TTP 21 s, AUC 1900 s, and MTT 38 s. Conventional US, colour Doppler, and CEUS features were suggestive of a malignant lesion. Histopathology (F) confirmed the features of invasive ductal carcinoma with infiltrating and pleomorphic tumour cells seen forming tubules
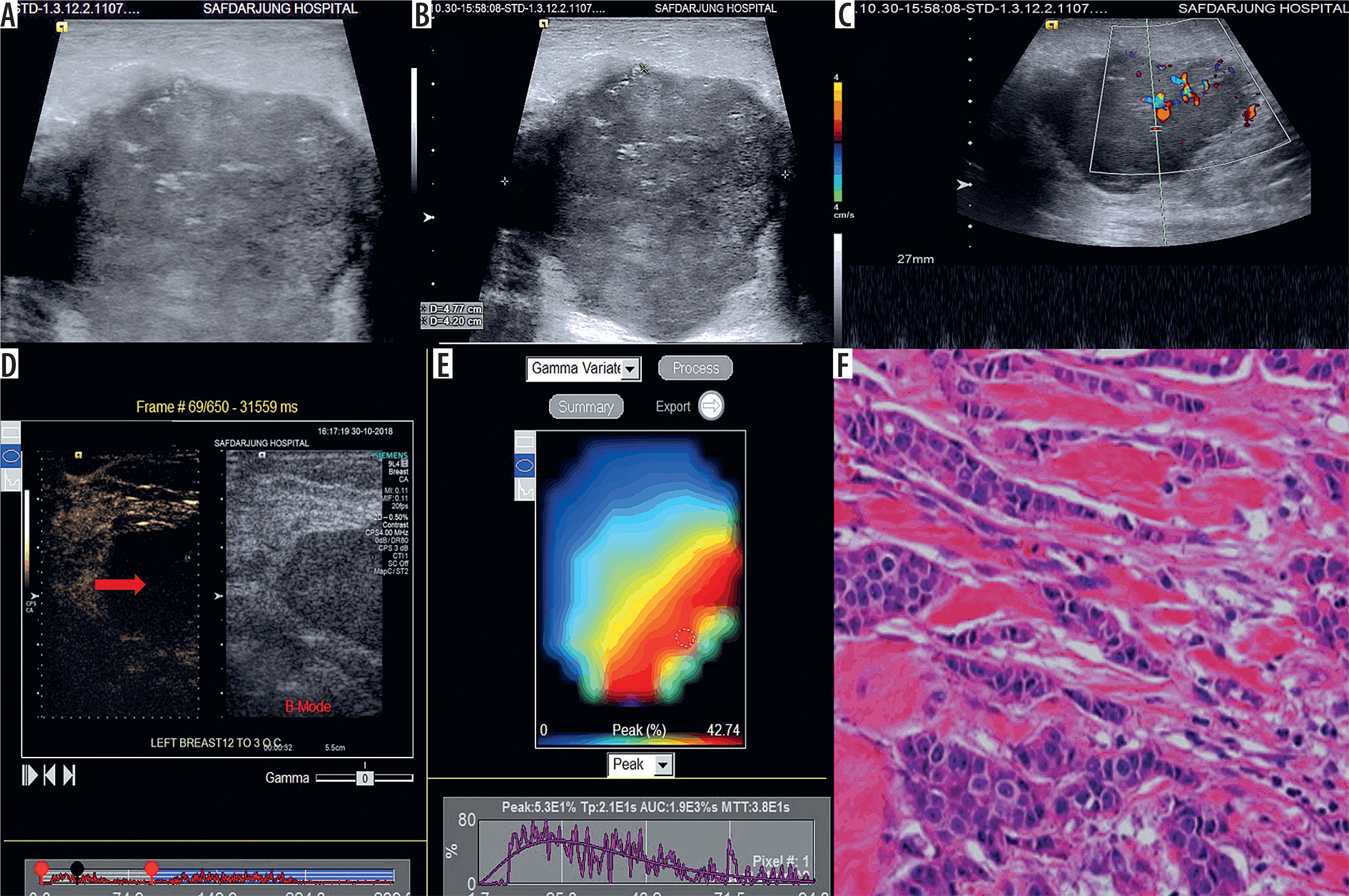
Figure 3
A-D shows grey-scale ultrasound (US), colour Doppler, contrast-enhanced ultrasound (CEUS), and histopathology image of a 35-year-old female patient who presented with a firm lump in her left breast. Grey-scale US (A) shows rounded mass in the 6 o’clock position of left breast with smooth macrolobulations. Internal echotexture was mainly homogeneous with a few linear branching lucencies. Colour Doppler (B) shows internal vascularity within the mass with RI and PI of 0.63 and 0.67, respectively. CEUS (C) revealed a homogeneously enhancing mass with few linear branching perfusion defects (green arrow) and regular margins (yellow arrow). The grey-scale US, colour Doppler, and CEUS features were suggestive of phyllodes tumour. Histopathology (D) confirmed benign phyllodes tumour with biphasic tumour with hypercellular stroma under cleft-like spaces lined by epithelium
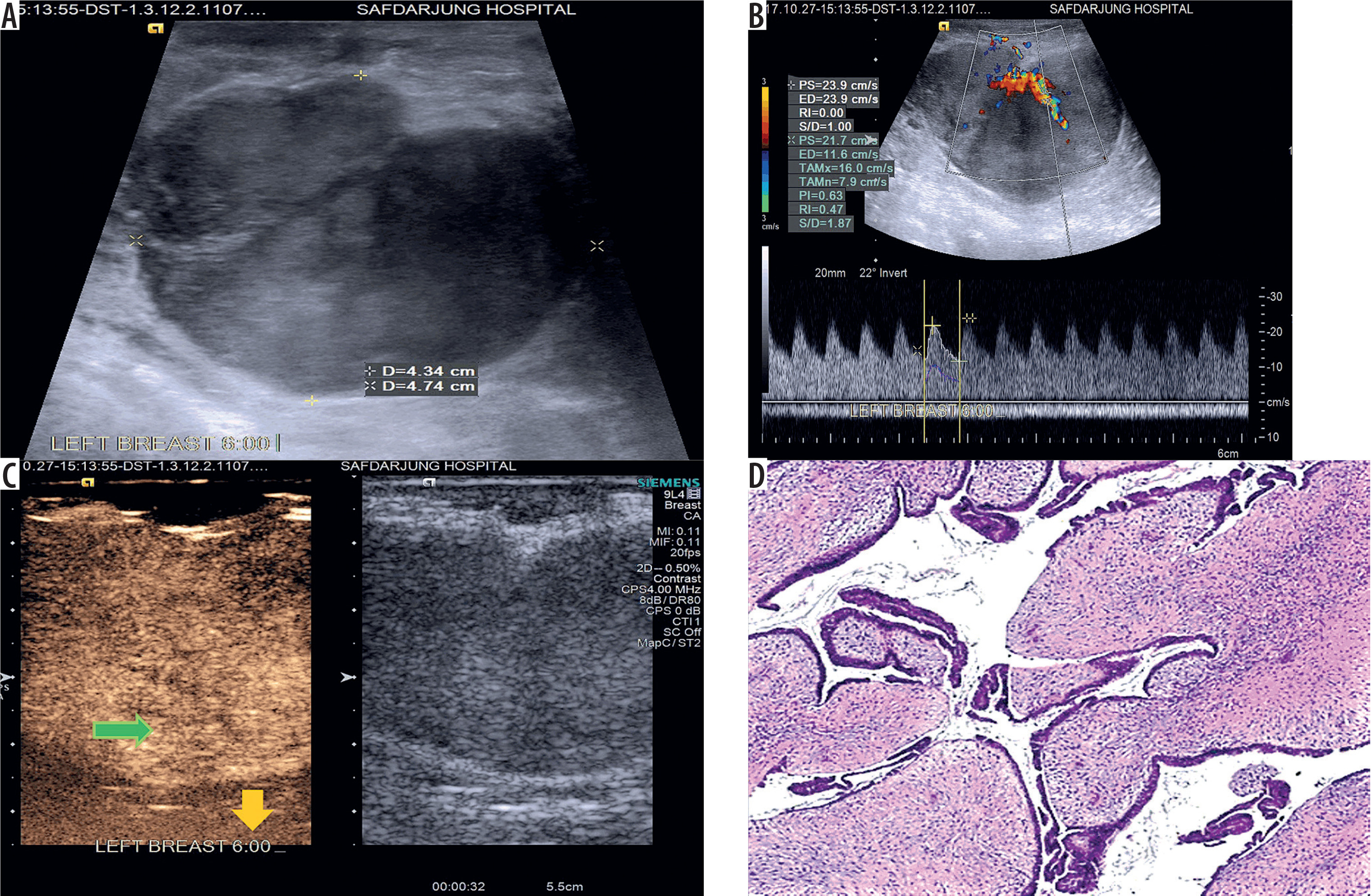
Figure 4
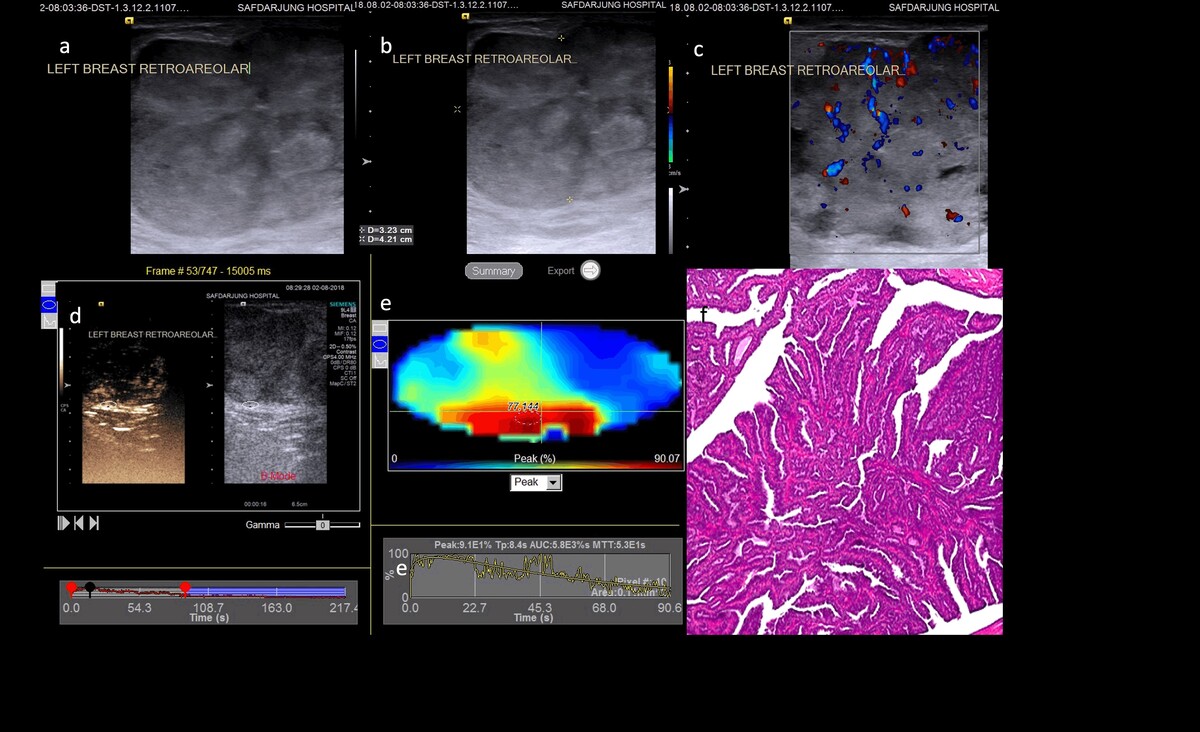
A-F shows grey-scale ultrasound (US), colour Doppler, and contrast-enhanced ultrasound (CEUS) study of a 48-year-old female patient who presented with a firm lump in her left breast. Grey-scale US (A, B) shows an oval hypoechoic mass with heterogeneous internal echotexture and regular margins in retroareolar region of the left breast. Colour Doppler (C) shows internal vascularity within the mass. CEUS (E) revealed heterogeneous enhancement with centripetal (order of) enhancement within the mass. Quantitative CEUS (E) shows PI 91%, TTP 8.4 s, AUC 5800 s, and MTT 53 s. Grey-scale US, colour Doppler, and CEUS findings were suggestive of low-grade malignancy. Histopathology (F), however, showed findings of intraductal papilloma with complex, intricate branching finger-like fronds within a dilated duct
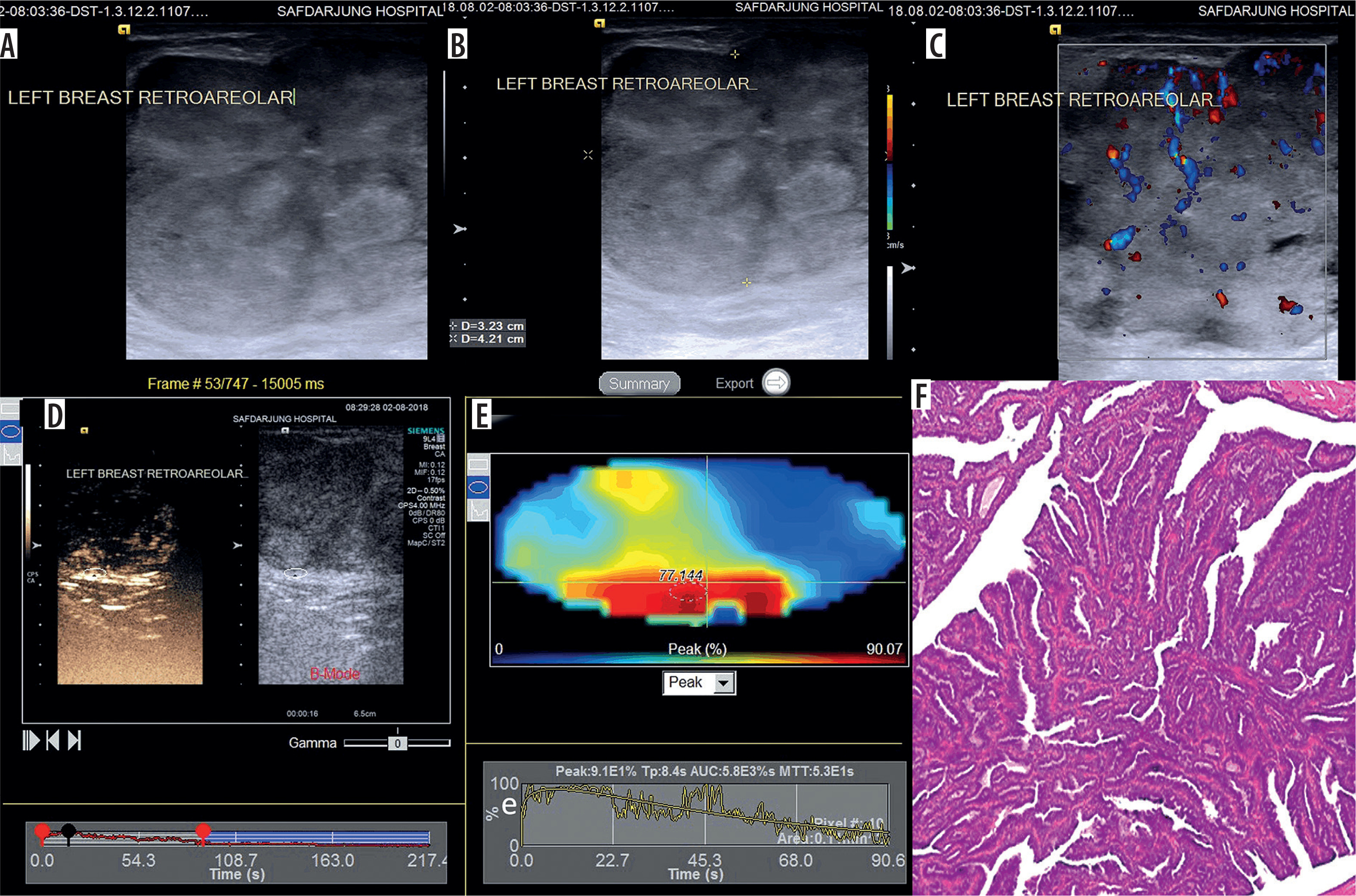
Figure 5
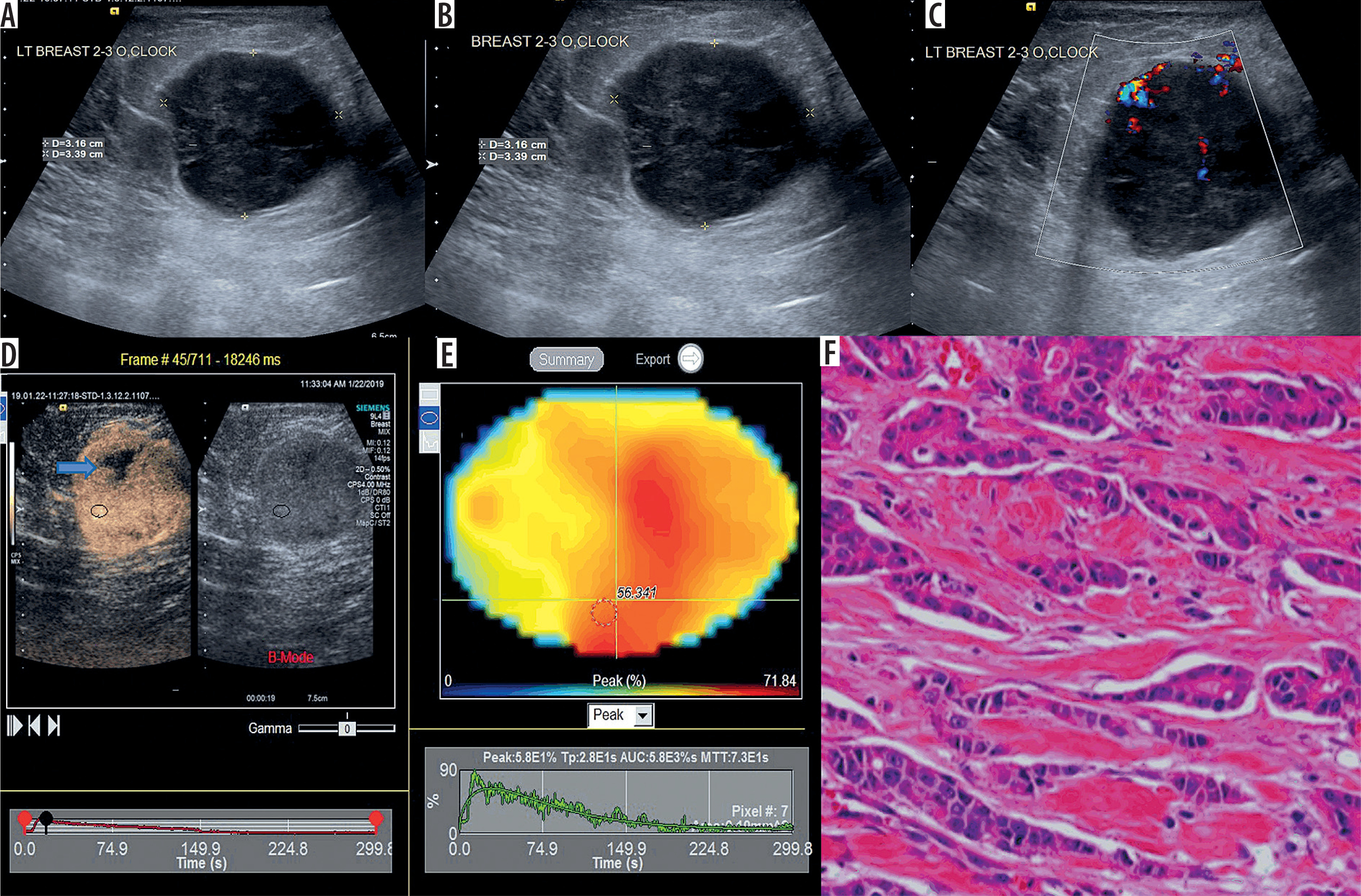
A-F shows grey-scale ultrasound (US), colour Doppler, and contrast-enhanced ultrasound (CEUS) study of a 41-year-old female who presented with firm lump in her left breast. Grey-scale ultrasound (A, B) shows a round hypoechoic mass with circumscribed margins in the 2 to 3 o’clock position in the left breast. Colour Doppler (C) shows internal vascularity within the mass lesion. CEUS (D) shows perfusion defect (blue arrow) with regular margin of enhancement in the mass. Quantitative CEUS (E) shows PI 58%, TTP 28 s, AUC 5800 s, and MTT 73 s. Conventional ultrasound and colour Doppler features were suggestive of low-grade malignancy. CEUS findings were also suggestive of low-grade malignant lesion. Histopathology (F) confirmed featured of invasive ductal carcinoma with infiltrating and pleomorphic tumour cells forming tubules
Discussion
The present study is significant because it found that CEUS had better diagnostic accuracy in comparison to diagnostic B-mode conventional US, along with Doppler. A 98.44% diagnostic accuracy with sensitivity of 100% and specificity of 96.15% were achieved by diagnostic CEUS.
In comparison, among other studies, Grewal et al. [10] reported that for distinguishing between benign and malignant lesions based on contrast enhancement patterns, the sensitivity and specificity were reported as 86.67% and 54.10%, 65%, respectively. When evaluating the presence of penetrating vessels as a criterion for malignancy, the sensitivity was 64%, and the specificity was 67.86%. A similar study by Luo et al. [6] reported that the sensitivity and specificity of CEUS for distinguishing between benign and malignant lesions were 84.4% and 87.8%, respectively.
In a systematic review and meta-analysis by Huang et al. [16] including 114 studies, CEUS demonstrated a pooled sensitivity of 89% and specificity of 85%. In another systematic review including 29 studies, to diagnose malignant breast lesions, CEUS carried a pooled sensitivity of 87% and specificity of 79% [9]. Tang et al. [12] also assessed the diagnostic accuracy of CEUS for differentiating malignant breast lesions and found that it carried a sensitivity of 89.4%, specificity of 65.3%, and diagnostic accuracy of 75.8%. The values were in line with the present study, indicating the diagnostic role of CEUS.
Moreover, CEUS diagnostic values outperformed the 89.06% diagnostic accuracy of B-mode US with colour Doppler, which had a sensitivity of 92.11% and specificity of 84.62%.
Among studies that assessed the diagnostic accuracy of B-mode US and colour Doppler, Watanabe et al. [17] reported that in differentiating benign from malignant breast lesions, the sensitivity of the combination of B-mode USG and colour Doppler was 94.7% and the specificity was 69.2%. In the study by Hashim et al. [18] for diagnosis of benign and malignant breast lesions, the sensitivity of B-mode USG with colour Doppler was 97.09%, and specificity was 80.65% – showing the superiority of diagnosing malignant breast lesions with CEUS.
In our study, it was seen that diagnostic CEUS did not miss any case of malignancy while it overdiagnosed one case of benign as false positive malignant. However, it held a significant κ-value of 0.967 and correlated well with histopathological diagnosis in comparison to diagnostic B-mode US with colour Doppler, which gave 4 cases as false positive malignant and missed 3 cases of malignancy, with a κ-value of 0.772.
Among other studies, Yuan et al. [19] compared conventional USG and CEUS in differentiating benign and malignant breast lesions. Taking pathological diagnosis as the reference standard, κ analysis revealed moderate agreement between conventional US and the gold standard (κ = 0.571), while CEUS showed a high level of agreement (κ = 0.875, p < 0.01). These findings indicate that CEUS may offer greater reliability than conventional US in distinguishing between benign and malignant breast lesions.
Overall, CEUS marks a notable improvement in diagnostic imaging techniques. Utilising blood-pool contrast agents, CEUS enables visualisation of lesion microcirculation – something that conventional colour Doppler USG might miss. Since the microcirculatory characteristics of breast lesions are closely linked to malignancy, CEUS provides valuable pathological insights. CEUS uses microbubble contrast agents and specialised imaging techniques to detect blood flow and tissue perfusion. The role of conventional imaging techniques is limited because it can only provide directional blood flow information and examine large blood vessels with high flow, while CEUS detects blood flow at the perfusion level. Breast cancer prognosis depends upon tumour growth and metastasis, which are directly linked to angiogenesis. CEUS analyses the microvascular architecture of tumour, which helps in differentiating benign and malignant masses [20].
Limitations
This study was conducted at a single centre, thus limiting the generalisation of the findings. Cases that did not undergo surgery and histopathological examination were not included. Use of contrast may remain a limitation for patients with drug allergies or contrast allergies.
Conclusions
CEUS demonstrated superior diagnostic performance in differentiating malignant from benign breast masses when compared with conventional B-mode US and colour Doppler imaging. CEUS achieved excellent agreement with histopathological findings, with a κ-value of 0.967 (p < 0.0001), and delivered high diagnostic metrics – including 100% sensitivity, 96.15% specificity, and an AUC of 0.98. Overall, CEUS exhibited outstanding diagnostic accuracy (98.4%) with high positive and negative predictive values, reinforcing its value as a reliable, non-invasive tool for characterising breast lesions and guiding clinical decision-making.