Introduction
Ureteroscopic lithotripsy (URSL) has become a core minimally invasive treatment for ureteral stones, particularly mid-to-lower segments, due to its high clearance rate and safety advantages [1]. However, postoperative infectious complications remain a serious clinical challenge. De la Rosette et al. [2] prospectively analysed 11,885 URSL patients and reported an infection rate of 2.8% with markedly increasing hospitalisation duration and septic shock risk, urinary tract obstruction is identified in up to 85% of urosepsis and shock cases [3], and the mortality of septic shock may reach 50% [4], emphasising the need for accurate infection risk stratification.
Current infection assessment relies primarily on preoperative urine culture, which is inadequate under obstructive conditions. Pyonephrosis patients present a culture-positive rate of only 49.3%, leaving nearly half of infections undetected [5]. Asymptomatic hydronephrosis without overt symptoms or NCCT findings also carries occult infection risk [6]. Established factors – operative time > 75 min, prolonged stent dwell (> 21 days), and renal stone location – have been confirmed as independent predictors after URSL [1]. Chronic kidney disease (CKD) is increasingly recognised as a critical risk factor [7]. Kim et al. [7] reported that CKD independently predicts febrile urinary tract infection following URSL, probably due to impaired tubular clearance and immune dysfunction that delay elimination of irrigation fluid and stone fragments, reducing resistance to pathogens. However, even when incorporating CKD, current models fail to identify all high-risk patients.
Recently, imaging-derived indicators such as renal pelvic urine density (RPUD), perinephric fat stranding, and the tissue rim sign have demonstrated predictive potential [7,8]. In infected states, renal pelvic urine exhibits elevated density due to bacteria, cellular debris, and inflammatory components [9]. RPUD effectively distinguishes simple hydronephrosis from pyonephrosis [10]. Multicentre studies further confirmed that elevated RPUD before extracorporeal shock wave lithotripsy (SWL) is strongly associated with severe postoperative infections; when RPUD ≥ 12 HU, sensitivity reaches 78.6% and specificity 85.9% [8]. However, data regarding RPUD in URSL remain insufficient, with existing evidence largely focused on SWL or retrograde intrarenal surgery (RIRS) [8,11]. Prior research has described computed tomography (CT) secondary signs of ureteral obstruction and their relation to stone characteristics [12], but these studies generally examined secondary signs alone and overlooked RPUD [7].
The combination of RPUD and CT secondary signs may yield superior predictive performance, particularly in CKD. CKD-related subclinical parenchymal injury may exacerbate obstructive physiology (elevated pelvic pressure and impaired urine clearance), making RPUD and perinephric fat stranding more reflective of occult infection [13]. Caglar et al. [11] reported RPUD as an independent predictor of post-RIRS infection, with stronger performance when combined with stone burden and body mass index (BMI) [11]. Extending this paradigm to URSL in CKD patients may fill a critical gap in current risk stratification.
Therefore, this study aims to evaluate the association between preoperative RPUD combined with CT-derived secondary signs and infectious complications in CKD patients undergoing URSL, to clarify their prognostic value and support individualised preventive strategies – such as early drainage or tailored antibiotic regimens – to reduce infection-related morbidity.
Material and methods
This retrospective cohort study was conducted at two tertiary hospitals, including patients who underwent URSL for ureteral stones between June 2015 and June 2025. The study population was derived from the hospital’s electronic medical record system. The study was designed in accordance with the Declaration of Helsinki and approved by the local Ethics Committee (No. 2025-K106-01).
Inclusion criteria
Inclusion criteria included patients aged > 18 years who underwent URSL for ureteral stones, and patients diagnosed with CKD [14]: (1) evidence of kidney damage (for ≥ 3 months) or (2) persistent reduction in glomerular filtration rate (GFR) < 60 ml/min/1.73 m2 for ≥ 3 months. Estimated GFR (eGFR) was calculated based on serum creatinine [14] (Table 1). Preoperative NCCT was available for assessment of stone characteristics and RPUD secondary signs. Complete clinical data (demographics, comorbidities, laboratory results, surgical records) and postoperative follow-up data (one month after the operation) were obtained.
Table 1
Formula for estimating adult glomerular filtration rate
Exclusion criteria
Exclusion criteria included the following: preoperative evidence of active infection (e.g., fever > 38oC, leukocytosis > 12,000 β/mm3); history of ureteral stent placement or nephrostomy before URSL; bilateral ureteral stones; and incomplete data on preoperative CT, laboratory tests, or postoperative outcomes. Clinical and radiographic data were extracted from electronic medical records. If the patient’s urine culture was positive before the operation, anti-infection treatment was administered until the urine culture turned negative, before proceeding with the surgical procedure.
Clinical data and CT scanning protocol and image analysis
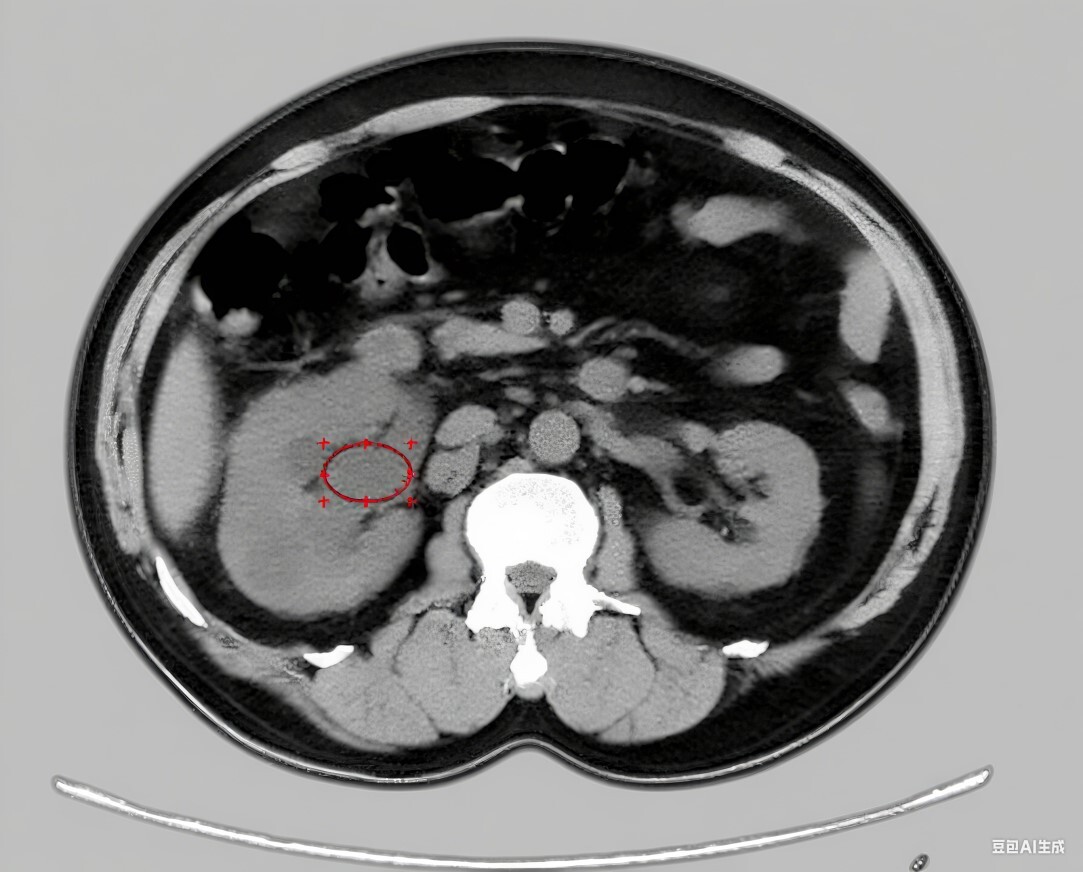
Preoperative CT imaging was performed using NCCT (Siemens Healthineers, Erlangen, Germany). Stone characteristics and RPUD secondary signs were evaluated using preoperative CT scans. Stone size was measured as the widest diameter on CT. Mid-upper ureteral stones were defined as those located between the ureteropelvic junction and the inferior margin of the sacroiliac joint. Conversely, lower ureteral stones were characterised as being situated between the inferior margin of the sacroiliac joint and the ureteral orifice in the bladder [15]. Stone density (in Hounsfield units, HU) was measured using a region of interest (ROI) encompassing the largest cross-sectional area of the stone (excluding adjacent soft tissue) on NCCT. Stone opacity was defined as opaque (visible on KUB) or non-opaque. RPUD was measured using preoperative NCCT. An ellipse-shaped ROI was drawn to cover the renal pelvis (excluding renal parenchyma, stones, and adjacent soft tissue) on axial images, and the mean HU value was recorded as RPUD (Figure 1). Secondary signs included hydronephrosis, perinephric fat stranding, periureteral fat stranding, and tissue rim sign (Figure 2). Perinephric fat stranding and periureteric fat stranding were defined as linear regions of soft tissue attenuation located in the perinephric space and periureteric space, respectively [7]. The positive tissue rim sign was defined as annular soft tissue attenuation (ranging from 20 to 40 HU), which results from the oedematous ureteral wall surrounding the stone [7]. Measurements were performed by 2 experienced radiologists; discrepancies were resolved by averaging the 2 values, and interobserver reliability was assessed using the intraclass correlation coefficient (ICC) ≥ 0.80. Preoperative bladder urine culture was collected ≤ 72 h before surgery. The degree of hydronephrosis was assessed using CT scan and was categorised in grades 1-4, as G1 (pelvic dilation only), G2 (pelvic + mild caliceal dilation), G3 (severe caliceal dilation), or G4 (caliceal dilation with renal parenchyma atrophy) [16].
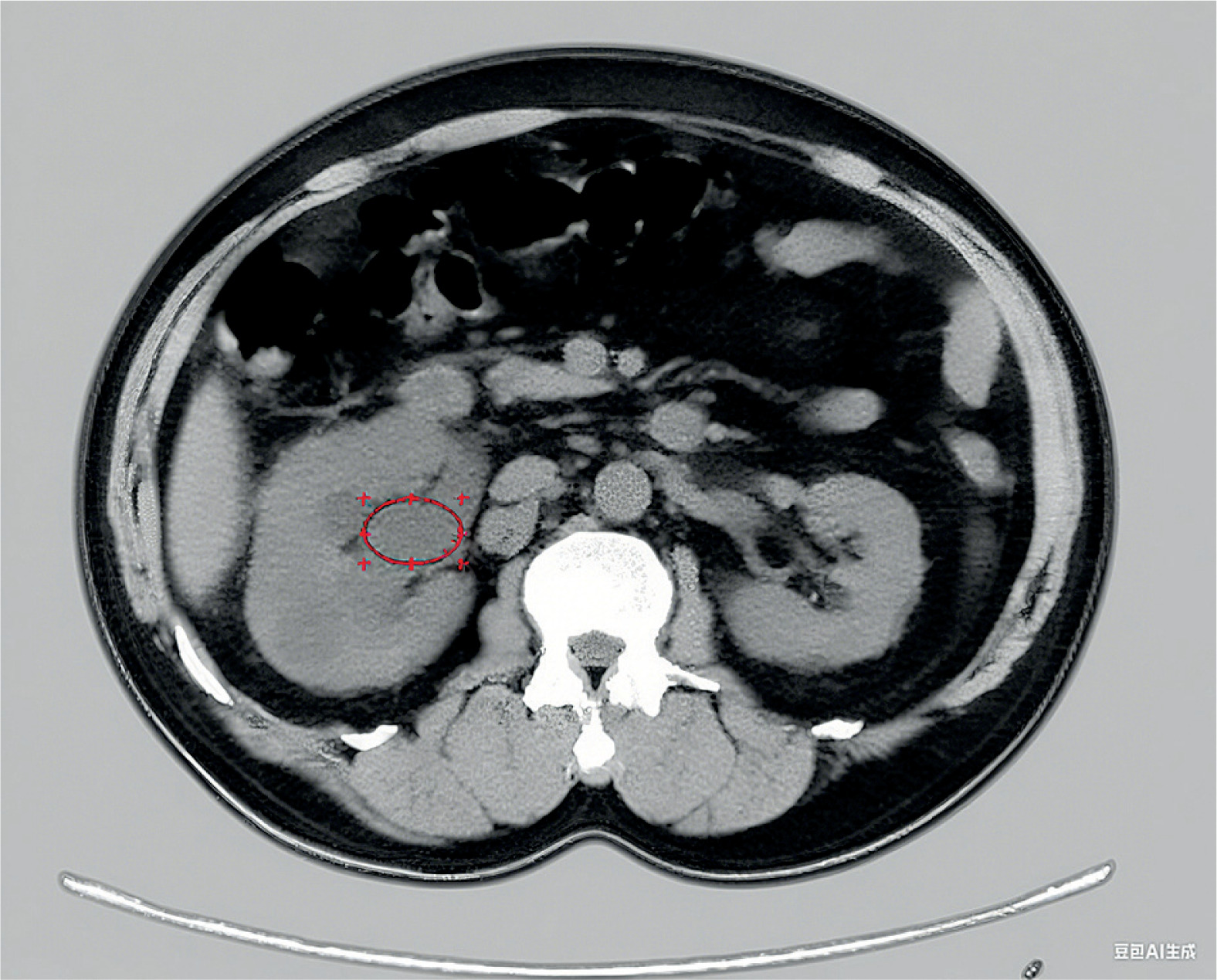
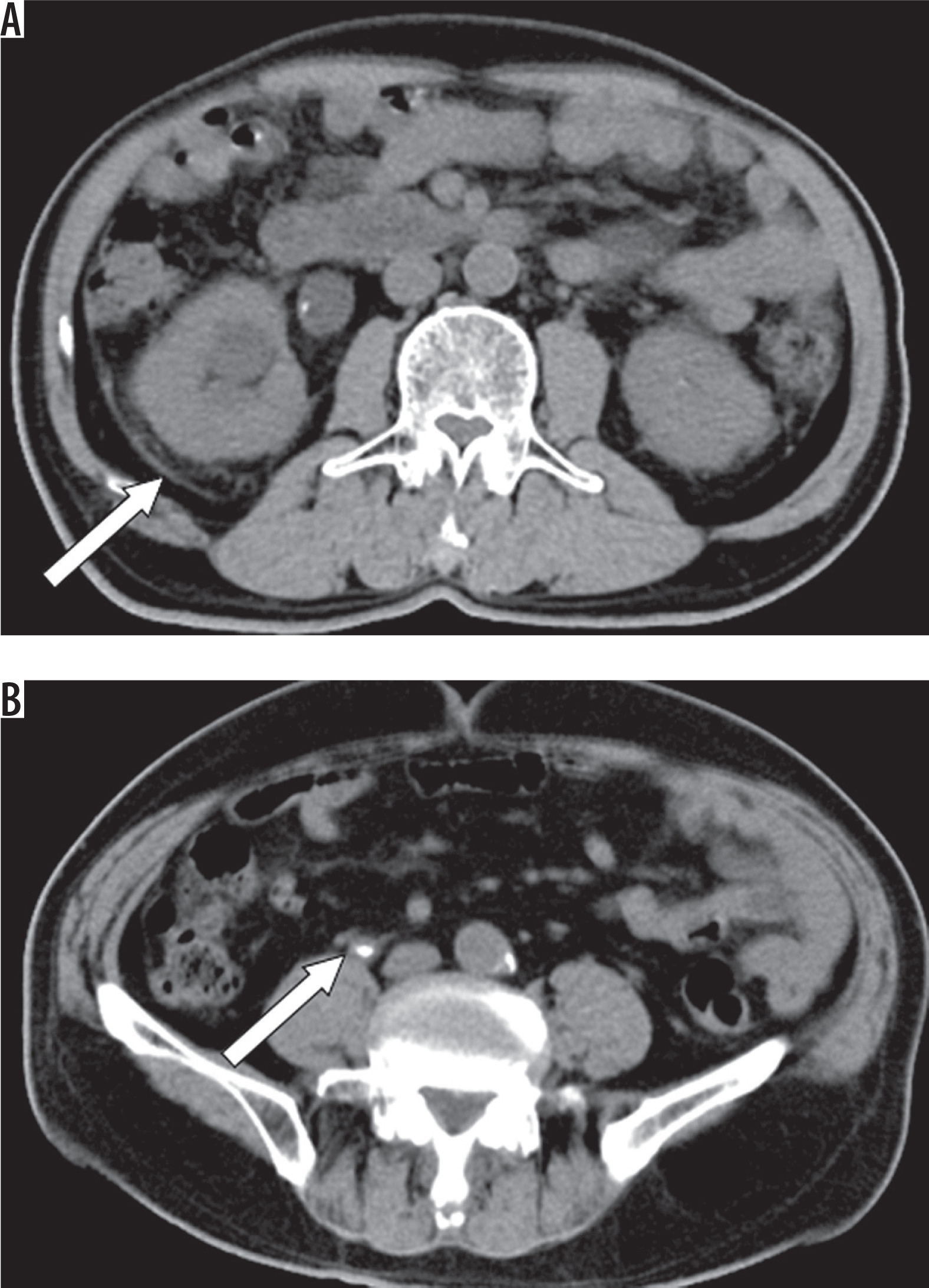
Figure 2
Features of perinephric fat stranding (A), and tissue rim sign (B) secondary to ureteral stone. The white arrows are pointing the perinephric fat stranding (A) and tissue rim sign (B)
Severe infectious complications, which occurred within one month after URSL, encompassed systemic inflammatory response syndrome (SIRS). SIRS was diagnosed when at least 2 of the following 4 criteria were met: (1) body temperature above 38oC or below 36oC; (2) heart rate greater than 90 beats per minute; (3) respiratory rate over 20 breaths per minute or a PaCO2 level lower than 32 mmHg (equivalent to 4.3 kPa); and (4) white blood cell count exceeding 12,000 cells/mm3, falling below 4000 cells/mm3, or containing more than 10% immature neutrophils [17].
Surgical technique
After induction of general anaesthesia, a ureteroscope (8/9.8 F, Wolf, Knittlingen, Germany) was introduced into the ureter under the guidance of a hydrophilic guidewire. A manual irrigation pump was used to improve visualisation during surgery, with low pressure maintained as much as possible. Then, ureteroscopy was performed under the guidance of the zebra guide wire until ureteral calculi were identified, and a single-use laser fibre and Ho: YAG laser device were used for lithotripsy with energy settings of 1.0–2.0 J at a pulse rate of 10–20 Hz. A 6F double J stent and Foley catheter were routinely placed at the end of the URSL. Patients were routinely given parenteral antibiotics for 3-5 days after URSL. If hydronephrosis was improved and no residual stone was found, the ureteral stent was removed under local anaesthesia in the fourth week after the operation.
Postoperative follow-up
The stone-free rate was assessed by postoperative imaging (NCCT) at one month, defined as no residual fragments or fragments < 4 mm [18].
Statistical analysis
Data were analysed using SPSS 26.0 (IBM Corp., Armonk, NY, USA). Continuous variables were reported as mean ± standard deviation for normally distributed data or median (interquartile range) for non-normally distributed data, and categorical variables were expressed as frequencies and percentages. Comparisons between the infectious and non-infectious groups were performed using the independent samples t-test or Mann-Whitney U test for continuous variables, and the c2 test or Fisher’s exact test for categorical variables. Variables with p < 0.05 in the univariate analysis were entered into a multivariate binary logistic regression model to identify independent predictors of postoperative infectious complications. Receiver operating characteristic (ROC) curves were constructed to evaluate the discriminatory performance of RPUD, and the area under the curve (AUC) was calculated. A multivariable predictive nomogram was constructed using R software (version 4.2.2; R Foundation for Statistical Computing, Vienna, Austria). Model performance was assessed using the concordance index (C-index) and calibration analysis. Internal validation was performed with 1000 bootstrap resamples to estimate optimism-corrected model performance and reduce overfitting. A two-tailed p-value < 0.05 was considered statistically significant.
Results
A total of 812 URSL patients were enrolled and divided into an infectious group (n = 102, 12.6%) and a noninfectious group (n = 710, 87.4%). No significant differences were found between the 2 groups in basic demographic characteristics (age, sex, BMI, ASA score), comorbidities (hypertension, coronary heart disease), stone-related features (localisation, opacity, density, laterality, previous stone surgery history, hydronephrosis), or postoperative stone-free rate (all p > 0.05) (Table 2).
Table 2
Comparison of patients’ demographic data and stone characteristics
Univariate analysis of post-URSL infection
Seven indicators showed significant differences (all p < 0.05): comorbidities – higher diabetes rate in the infectious group (33.3% vs. 17.5%, p < 0.001); stone size – larger mean diameter in the infectious group (16.5 ± 4.2 mm vs. 13.9 ± 3.8 mm, p < 0.001); preoperative infection – higher positive rate of preoperative bladder urine culture in the infectious group (36.3% vs. 11.0%, p < 0.001); operative time – longer in the infectious group (55.7 ± 16.3 min vs. 46.4 ± 16.1 min, p = 0.002); postoperative hospital stay – longer in the infectious group (5.6 ± 2.4 days vs. 2.8 ± 2.1 days, p < 0.001); RPUD – higher in the infectious group (13.7 ± 4.8 HU vs. 8.5 ± 3.7 HU, p < 0.001); and CT secondary signs – higher incidence of perinephric fat stranding (31.4% vs. 22.1%, p = 0.039) and tissue rim sign (25.5% vs. 17.2%, p = 0.042) in the infectious group (Table 2).
Multivariate analysis of post-URSL infection
Multivariate logistic regression identified 7 independent risk factors (all p < 0.05): diabetes – 4.232-fold higher infection risk (OR = 4.232, 95% CI: 2.143-8.357, p < 0.001); stone diameter – 19.6% higher risk per 1 mm increase (OR = 1.196, 95% CI: 1.106-1.293, p < 0.001); positive preoperative bladder urine culture – 6.174-fold higher risk (OR = 6.174, 95% CI: 3.012-12.654, p < 0.001); operative time – 5.3% higher risk per 1 min increase (OR = 1.053, 95% CI: 1.032-1.073, p < 0.001); RPUD – 38.5% higher risk per 1 HU increase (OR = 1.385, 95% CI: 1.282-1.497, p < 0.001); perinephric fat stranding – 2.356-fold higher risk (OR = 2.356, 95% CI: 1.180-4.706, p = 0.015); and tissue rim sign – 2.268-fold higher risk (OR = 2.268, 95% CI: 1.127-4.565, p = 0.022) (Table 3).
Table 3
Multivariate analysis of factors related to the development of postoperative infection
Prediction model for post-URSL infection
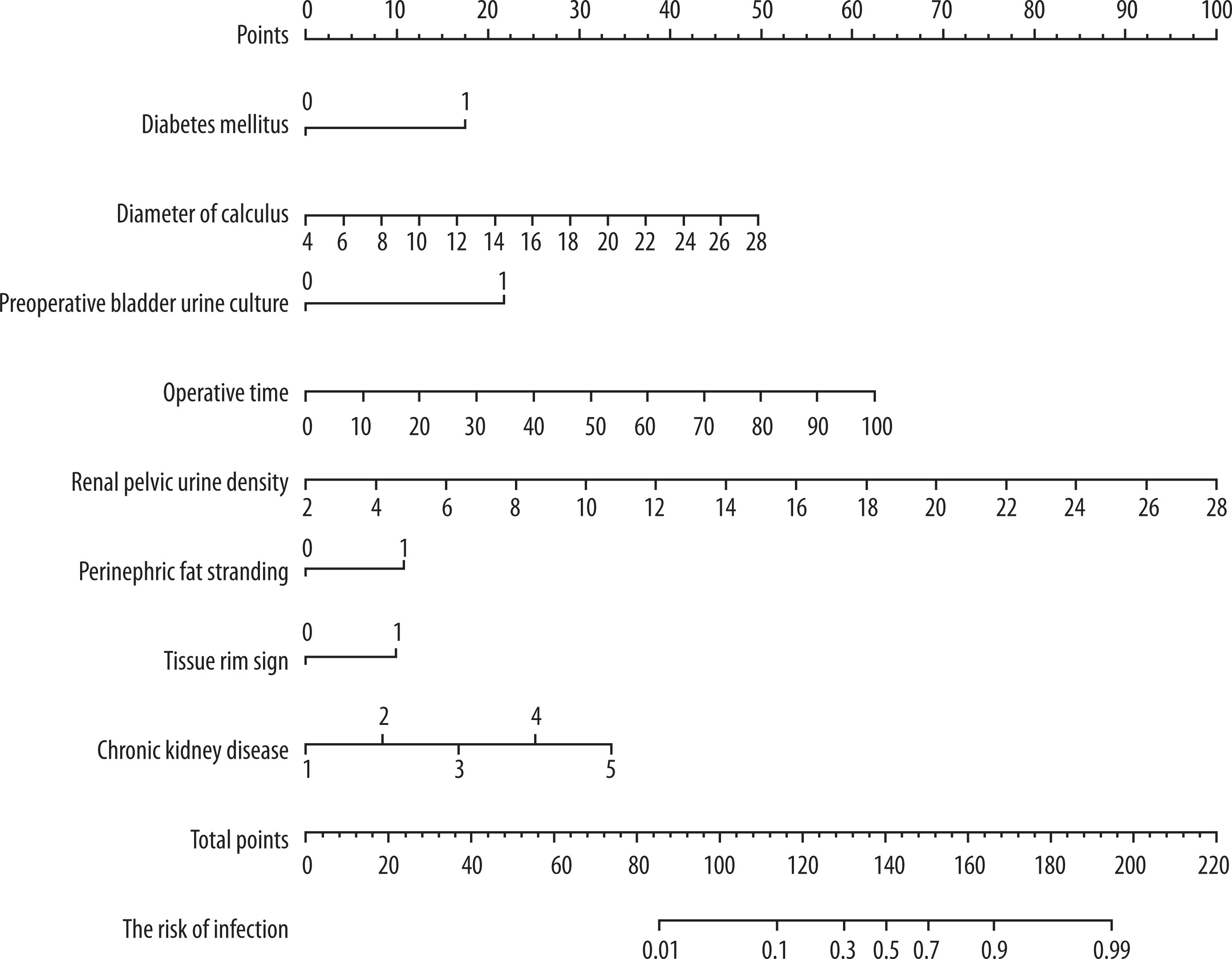
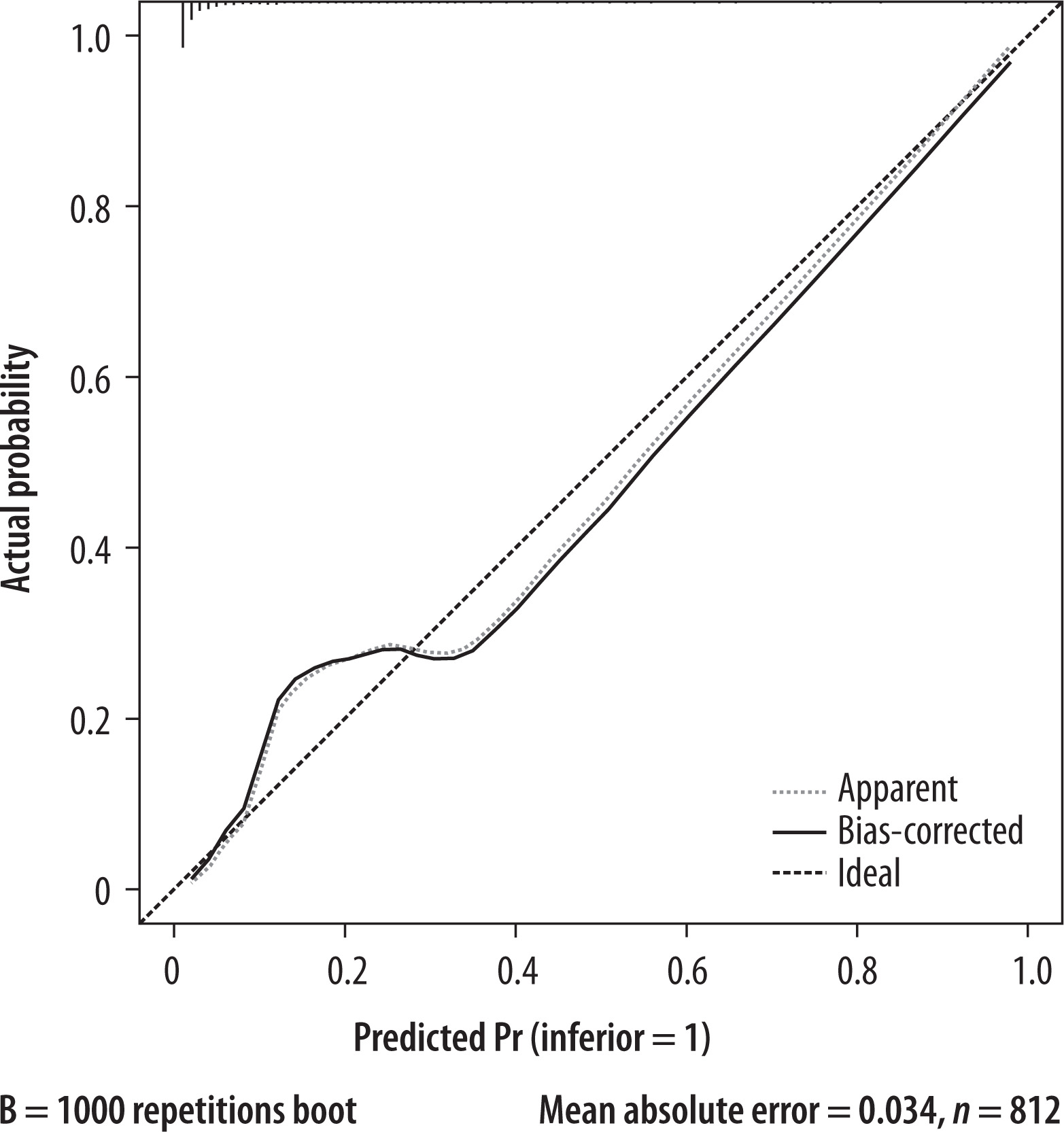
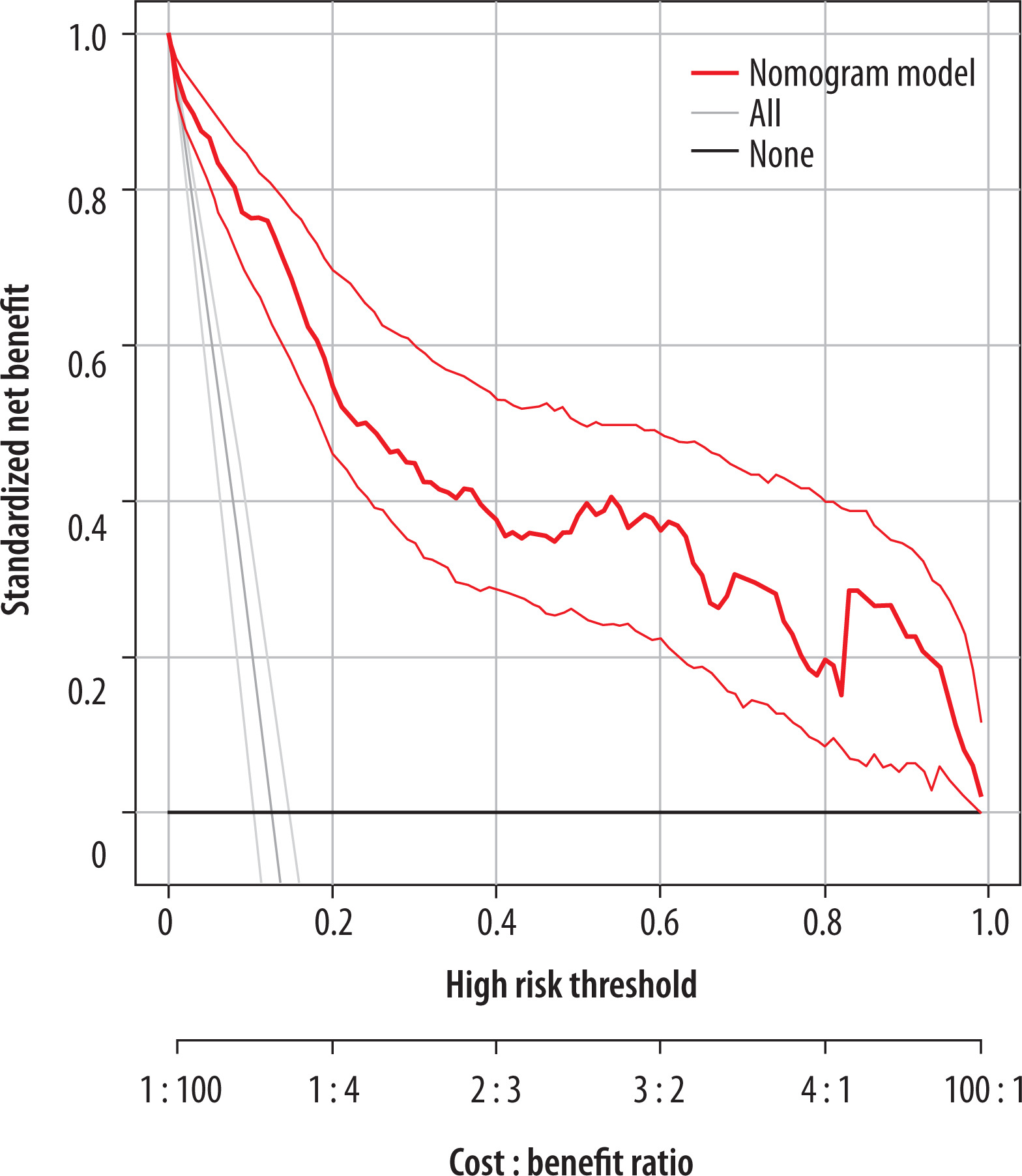
The multifactorial prediction model (incorporating 7 risk factors) had an AUC of 0.932 (p < 0.001, Figure 3) and a c-index of 0.932, showing excellent discriminative ability. A nomogram (Figure 4) was built for individual infection probability prediction, and the calibration curve (Figure 5) demonstrated good agreement between predicted and observed rates. A specialised predictive model for CKD patients was also developed via decision curve analysis (Figure 6).
Figure 3
ROC curves for predicting postoperative infectious complications after ureteroscopic lithotripsy with chronic kidney disease: multifactorial model
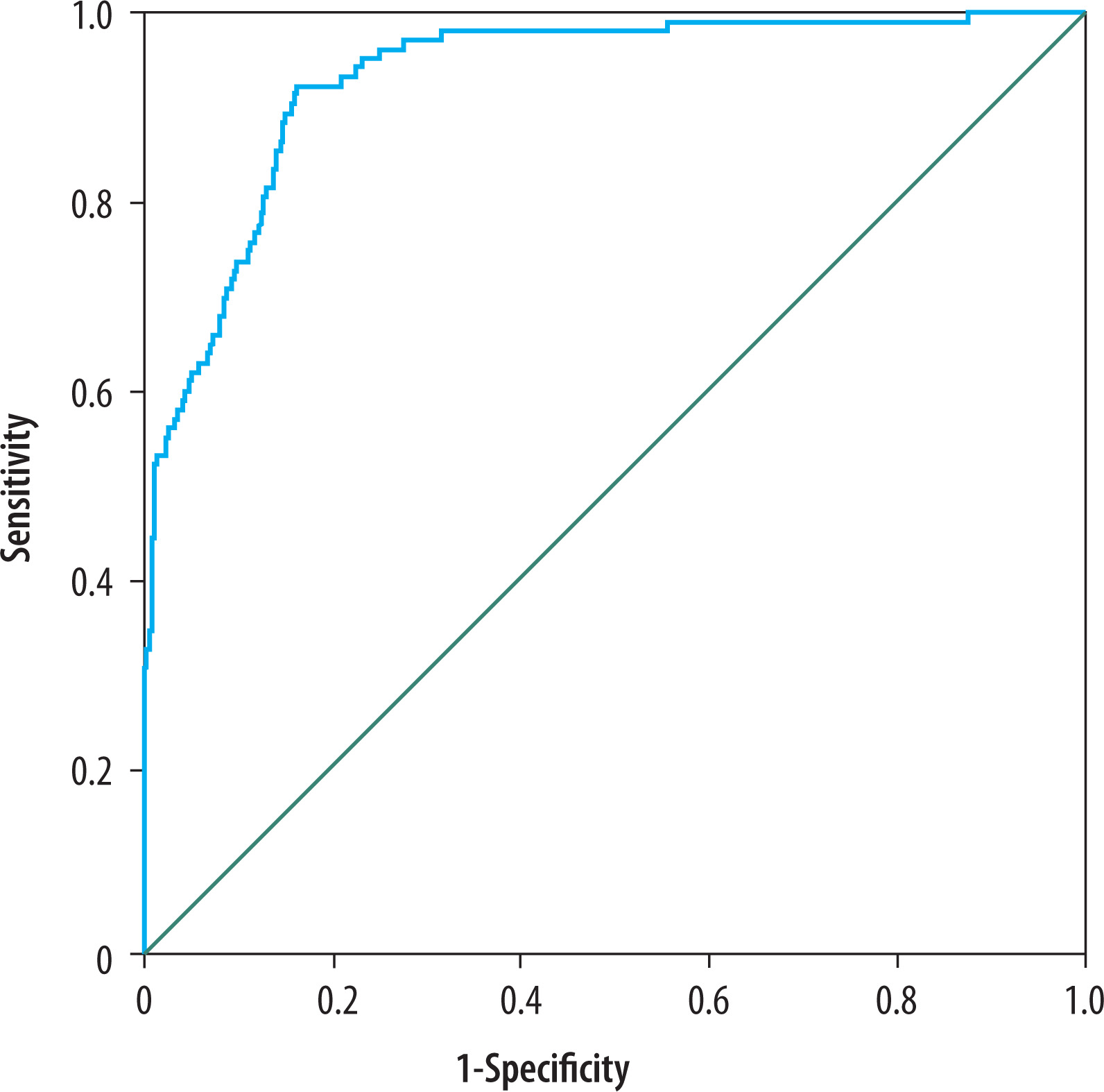
Figure 4
Nomograms for infection in the patient with chronic kidney disease after ureteroscopic lithotripsy
Discussion
In this two-centre retrospective cohort including 812 patients undergoing URSL for ureteral calculi, we demonstrated that elevated RPUD on preoperative NCCT, together with CT-derived secondary signs – perinephric fat stranding (PFS) and the tissue rim sign (TRS) – is independently associated with postoperative infectious complications, particularly in patients with CKD. To our knowledge, this is the first study to systematically evaluate the combined predictive value of RPUD and secondary signs in the specific context of CKD undergoing URSL, thereby extending existing evidence primarily derived from SWL or RIRS studies. Our findings highlight that radiologic markers reflecting obstructive physiology and occult infection may significantly improve preoperative risk stratification beyond traditional clinical and laboratory indicators.
Postoperative infection following URSL remains a relevant and potentially life-threatening complication. De la Rosette et al. [2] reported a 2.8% infection rate in a global multicentre cohort of 11,885 URSL procedures, demonstrating the profound impact of infectious events on morbidity and hospitalisation. Urosepsis may arise in up to 85% of cases with obstructive uropathy [3], and mortality can approach 50% [4]. Despite the recognised importance of infection prevention, current clinical practice still relies heavily on preoperative bladder urine culture. However, its diagnostic reliability is limited in the presence of obstruction, where proximal infected urine may remain isolated from the bladder. Prior work shows that only 49.3% of pyonephrosis cases have positive bladder cultures [5], and even patients with asymptomatic hydronephrosis may harbour occult infection [6]. This diagnostic gap is particularly relevant in CKD, where impaired immune function, tubular dysfunction, and chronic inflammatory milieu further amplify infection susceptibility [7,19,20].
The present study identifies RPUD as a robust and independent predictor of postoperative infection. RPUD reflects the attenuation of renal pelvic urine, which increases in the presence of bacterial colonisation, inflammatory debris, and concentrated cellular components [21]. Yuruk et al. [10] demonstrated that RPUD differentiates pyonephrosis from simple hydronephrosis with high accuracy. Liu et al. [8] later confirmed, in a multicentre SWL cohort, that increased RPUD correlates linearly with severe postoperative infections, with RPUD ≥ 12 HU exhibiting high specificity. Our findings extend these observations to URSL and specifically to high-risk CKD patients. The lower RPUD threshold observed in our study (mean 13.7 HU in infected vs. 8.5 HU in noninfected cases) suggests that even modest increases in pelvic attenuation may reflect clinically significant infection in CKD, whose compromised renal clearance may limit the ability to eliminate pathogens or inflammatory products [7,19].
CT secondary signs also demonstrated significant predictive value in our cohort. PFS and TRS signify increased perinephric pressure, lymphatic congestion, and ureteral wall oedema caused by persistent obstruction [7,12]. These imaging markers capture the local tissue response to elevated intrapelvic pressure – an environment conducive to bacterial proliferation and pyelovenous or pyelolymphatic reflux during endoscopic irrigation [22]. In URSL, intraoperative irrigation increases the likelihood of bacteraemia when microscopic or subclinical infection is present. This mechanism is exacerbated in CKD, where impaired host immunity and altered renal microenvironment facilitate pathogen dissemination [19]. Our multivariate analysis confirms that PFS (OR = 2.356) and TRS (OR = 2.268) significantly increase the risk of infectious complications, indicating their relevance as noninvasive markers of occult upper tract inflammation.
When considered together, RPUD and secondary signs provide a more comprehensive assessment of infection risk than traditional factors alone. Prior studies have identified positive urine culture, prolonged operative time, large stone burden, stent dwell time, and renal stone location as risk factors for post-URS infection [1,9]. While our results confirm several of these associations, RPUD and secondary signs offer unique advantages: (1) they are readily available from routine preoperative NCCT, (2) they directly reflect the pathophysiological changes occurring in obstructed, potentially infected systems, and (3) they are especially informative when bladder cultures are negative – a common situation in both obstructive uropathy and CKD [5].
The predictive model derived from our multivariate analysis exhibited excellent discrimination (AUC = 0.932), suggesting substantial clinical utility. This model may guide preoperative decision-making, including intensified antibiotic prophylaxis, pre-URS drainage with ureteral stent or nephrostomy, and intraoperative pressure-controlled irrigation. Such individualised strategies are particularly relevant for CKD patients, who experience disproportionately severe infectious outcomes [7]. Our findings therefore align with recent evidence supporting radiologic-based risk stratification as an emerging tool in endourology.
Study limitations
This study has several limitations. First, the retrospective design and restriction to two centres may introduce selection bias and limit generalisability. Second, we did not compare RPUD with renal pelvic urine or stone cultures, which have been shown to better predict postoperative sepsis than bladder cultures [23]. Third, irrigation pressure during URSL was not standardised, potentially influencing the relationship between RPUD and infection. Finally, although internal validation using bootstrap resampling improves reliability, external validation across different populations and imaging platforms remains necessary before broad implementation. Future prospective studies should investigate the biological correlates of RPUD, integrate serum biomarkers such as CRP or procalcitonin [24], and explore the interaction between RPUD and stone composition, particularly struvite stones.
Conclusions
Our findings highlight the clinical relevance of RPUD and CT secondary signs as noninvasive, readily accessible predictors of infectious complications following URSL, especially in CKD patients. Incorporating these imaging features into preoperative assessment may enhance risk stratification, support individualised perioperative management, and ultimately improve patient outcomes in this vulnerable population.