Introduction
Breast cancer is the most common malignancy in women and a significant cause of morbidity and mortality worldwide [1]. Among the imaging methods used in diagnosis and staging, magnetic resonance imaging (MRI) stands out, particularly due to its high sensitivity [2]. Dynamic contrast-enhanced breast MRI plays a critical role in distinguishing malignant from benign lesions by providing both morphological and functional information. However, despite its high sensitivity, MRI’s relatively low specificity can lead to false-positive and false-negative results [3].
The Breast Imaging Reporting and Data System (BI-RADS), widely used in clinical practice, provides a standard terminology for describing breast lesions. However, BI-RADS interpretation involves significant subjectivity, particularly among inexperienced radiologists, increasing the risk of misclassification [4]. To overcome these limitations, the Kaiser score (KS) was developed by Baltzer and colleagues in 2013. It is a decision tree algorithm that incorporates five main parameters derived from BI-RADS criteria (root sign, margin features, contrast patterns, time-intensity curve, peritumoral edema) [2]. The KS improves diagnostic accuracy in both experienced and inexperienced radiologists as a clinical decision support tool and can reduce unnecessary biopsies [5,6]. Recent systematic reviews and meta-analyses have shown that the KS achieves high sensitivity (95%) and specificity (70%) in detecting malignant lesions and offers more balanced diagnostic performance compared to BI-RADS [6]. However, false-negative results may occur, particularly in small lesions (≤ 1 cm), specific histopathological subtypes such as intraductal papilloma and mucinous carcinoma, or in the presence of prominent background parenchymal enhancement (BPE) [7,8]. The current literature indicates that identifying factors associated with false-negative KSs in detail will both optimize clinical decision-making processes and contribute to the proper integration of multimodal imaging approaches.
The aim of this study was to evaluate the KS on MRI in patients diagnosed with breast cancer and to determine the clinical, pathological, and radiological factors that lead to false-negative KSs.
Material and methods
Patient selection
This study has been approved by the Institutional Review Board, and the requirement for written informed consent has been waived (decision date: 10/22/2025 and decision no: 2025/497). Breast MRIs performed at our hospital between January 2024 and January 2025 were retrospectively reviewed. Patients diagnosed with breast cancer histopathologically and whose mammography images were available were included in the study. Patients with low diagnostic adequacy of mammography or MRI and those unsuitable for evaluation, patients with a history of radiotherapy in the same breast, and patients whose histopathological results could not be obtained were excluded from the study. In cases of multiple lesions, the lesion confirmed by biopsy was evaluated. Non-mass enhancement (NME) lesions were excluded to maintain a homogeneous cohort because several KS components rely on mass-specific morphological descriptors (e.g., margin-related features), which may be less applicable or differently interpreted in NME.
Imaging technique and image analysis
MRI was performed in the prone position using an 8-channel breast coil on a 1.5 Tesla MRI scanner (Signa Voyager, GE HealthCare, USA). Axial and sagittal fat-suppressed T1-weighted pre-contrast images and axial T2-weighted images were obtained in all MRI scans. Axial diffusion-weighted images (DWI) were also obtained at b-values of 0, 400, and 800 s/mm2. Apparent diffusion coefficient (ADC) maps were automatically generated on the operating console using the least squares method with all three images and b-values of 0, 400, and 800 s/mm2. After intravenous injection of 0.1 mmol/kg body weight gadolinium contrast medium (Gadoteric acid, Dotarem, Guerbet), 5 dynamic post-contrast fat-suppressed T1-weighted images (TR: 7 ms, TE: 2.2 ms, 1.4 mm thickness, matrix 512 × 512, field of view 350, flip angle 10°) were obtained. Dynamic curves of percent enhancement versus time were obtained for lesions at small regions of interest, positioned on the brightest portion of the lesion.
Image analysis was performed by a breast radiologist with 10 years of experience. The reader was blinded to histopathological results at the time of KS assignment. BPE was categorized as mild (minimal and mild according to the BI-RADS MRI dictionary) or distinct (moderate and marked). The largest tumor size was measured and recorded on MRI. Lesions were graded from 1 to 11 according to KS as defined in the literature [2]. A cutoff of KS ≥ 5 was selected in accordance with commonly used KS-based diagnostic thresholds reported in prior validation studies; lesions with KS ≥ 5 were considered positive, whereas those with KS < 5 were considered false-negative in this cancer-only cohort (Figure 1: 1 = lowest, very low probability of cancer; 11 = highest, very high probability of cancer). The presence of diffusion restriction and ADC values were recorded in DWI. Dynamic curves of percent enhancement versus time were obtained using small regions of interest (ROIs) positioned on the most intensely enhancing solid portion of the lesion on post-contrast images. Areas of necrosis/cystic change, hemorrhage, and macroscopic fat were avoided. ROI location was matched to the corresponding ADC map to record ADC values from the same solid tumor component. Mammography findings were available during the MRI evaluation.
Figure 1
Flowchart of the Kaiser score. This flowchart is adapted from [2]. TIC – time-signal intensity curve

Standard mammography was performed in the craniocaudal and mediolateral oblique positions (Senographe Pristina, GE Healthcare, USA). Mammograms obtained from other centers were accepted if the image quality was adequate. The presence of suspicious microcalcifications (amorphous, coarse heterogeneous, fine pleomorphic, fine linear, or fine-linear branching) according to BI-RADS was recorded on mammography.
Histopathological evaluation
Histopathology reports were retrospectively reviewed for estrogen receptor (ER), progesterone receptor (PR), histological grade, Ki-67 value, HER2 receptor status, and histological type. Nuclear staining ≥ 10% was considered ER and PR positive. For HER2 status, 3+ staining and/or a positive HER2 gene amplification test were considered positive, while 0 or 1+ staining was considered negative. For the Ki-67 index, nuclear staining of > 14% was considered high. Based on these criteria, the molecular subtypes were classified as luminal A, luminal B, HER2-positive, and triple-negative.
Statistical analysis
IBM SPSS Statistics 26.0 software (IBM Corp., Armonk, NY, USA) was used for data analysis. In the comparative analysis, the two-sample t-test or Wilcoxon rank sum test was used for continuous variables, and the c2 test or Fisher’s exact test was used for categorical variables. In univariate analysis, the odds ratio (OR), 95% confidence interval (CI), and p-values were calculated for each variable using Fisher’s exact test. Subsequently, a simplified multivariate logistic regression model was constructed using variables with p < 0.1 in the univariate analysis. In this model, the independent effects of the variables were reported with OR, 95% CI, and p-values. The level of statistical significance was set at p < 0.05 for all tests.
Results
A total of 120 breast masses from patients were included in the study. In 111 of these cases (92%), the KS was 5 or above and yielded a true-positive result. In 9 cases (8%), the score was below 5 and yielded a false-negative result. Cases 2 and 6 showing false-negative KS are shown in Figures 2 and 3, respectively. The analysis of lesions in the false-negative group is given in Table 1.
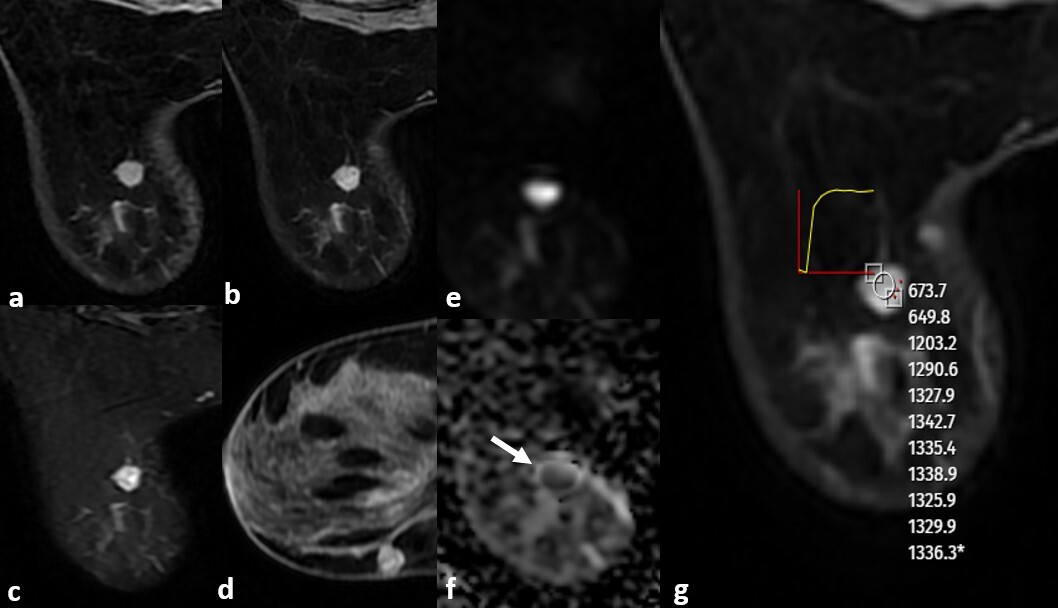
Figure 2
An 8 mm diameter, well-defined, round lesion visible on magnetic resonance imaging of a 40-year-old female patient who presented for a routine breast examination, showing contrast-enhanced (A) and non-contrast-enhanced axial and sagittal (B, D) T1-weighted images. The lesion showed heterogeneous enhancement on T1-weighted images, was hyperintense on fat-suppressed T2-weighted images (C), demonstrated diffusion restriction on diffusion-weighted imaging (E, F), and exhibited a plateau enhancement pattern on dynamic contrast-enhanced T1-weighted images (G). The Kaiser score was assessed as 2. Core needle biopsy revealed luminal A, HER2-negative Grade 1 invasive ductal carcinoma

Figure 3
A 38-year-old female patient with a history of breast cancer had a mass detected on physical examination. Ultrasonography revealed a well-defined, oval, hypoechoic solid mass. Core needle biopsy revealed luminal B, HER2-positive Grade 2 invasive ductal carcinoma. Preoperative MRI (A) T1-weighted pre-contrast, C) fat-suppressed T2-weighted image, B, D) post-contrast axial and sagittal T1-weighted images, E) dynamic contrast-enhanced T1-weighted images revealed a 19 mm circumscribed, homogeneously enhancing mass with a plateau enhancement pattern and a Kaiser score of 2
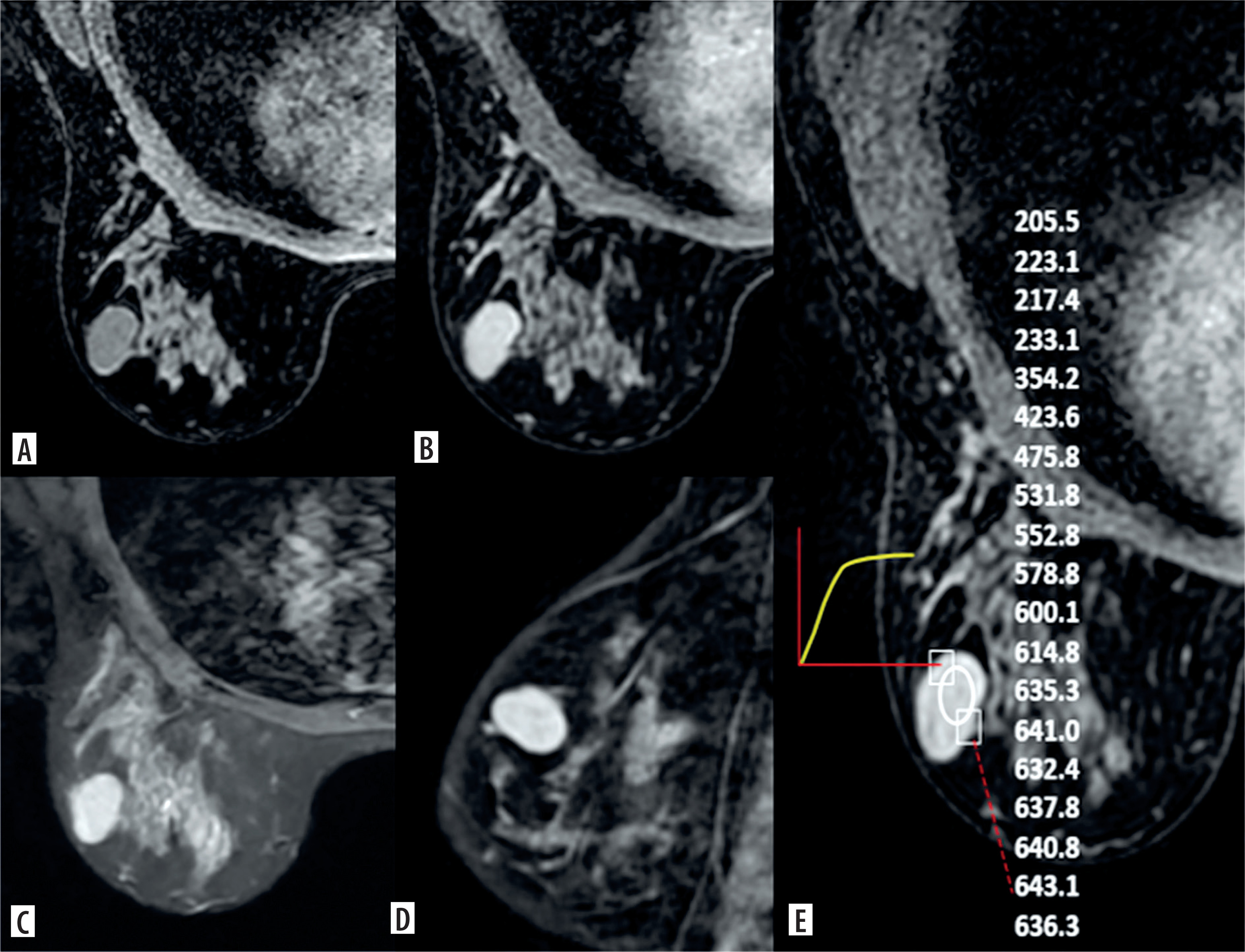
Table 1
Characteristics of lesions with false-negative Kaiser scores
The mean age was 57.6 (min: 28, max: 91), and there was no difference between the groups. According to the KS, 33.3% (3/9) of patients in the false-negative group and 3.6% of true-positive patients had a history of breast cancer, and a statistically significant difference was found between the groups (p = 0.009). No difference was found in the rates of suspicious microcalcifications detected on mammography (p = 0.889). Tumor size on MRI was statistically significantly lower in the false-negative group compared to the true-positive group (p = 0.002). No significant differences were found between the groups in terms of other MRI features.
When the groups were compared in terms of histopathological features, the histological type was found to be statistically significantly different (p = 0.035). The rates of invasive ductal carcinoma were similar between groups (66.7% vs. 67.6%). However, 23.4% (26/111) of the true-positive group had invasive lobular carcinoma (ILC) histology, while no ILC was detected in the false-negative group. No statistically significant differences were found between the groups in terms of ER/PR positivity, histological grade, HER2 receptor status, Ki-67 index, and molecular subtypes. Detailed analysis is shown in Table 2.
Table 2
Comparison of histopathological and imaging results between true-positive and false-negative groups
According to univariate regression analysis, a history of breast cancer, tumor size less than 2 cm, and HER2 positivity were found to be statistically significantly associated with false-negative KSs (Table 3). In the multivariate analysis performed with the variables found to be significant in the univariate analysis, only tumor size was found to be associated with false-negative KS (p = 0.018).
Table 3
Univariate and multivariate analysis results
Discussion
This study examined the clinical, radiological, and pathological factors associated with false-negative results of the KS in breast MRI. The false-negative rate was determined to be 8% in our study, which was consistent with rates reported in the literature [8,9]. A history of breast cancer in the patient, small lesion size (< 2 cm), and HER2 positivity were found to be associated with a false-negative KS score.
In our study, only small tumor size was identified as a statistically independent predictor in multivariate analysis and was found to be the strongest predictor of false-negative KSs. An OR < 1 for tumor size indicates an inverse association with false-negative KS; therefore, smaller lesions are more likely to yield a false-negative KS classification. In a study by Avdan Aslan et al. [8], small tumors were also identified as an independent risk factor for false negativity. A study involving 316 breast lesions showed that malignancy could be largely ruled out in lesions with a KS < 5, and six false-negative lesions with a tumor size < 1 cm were reported [9]. Zhang et al. [7] reported that, in addition to small tumor size (< 1 cm), the presence of marked BPE and T2 hyperintensity may also contribute to false negatives. In contrast, some studies in the literature have also shown that the presence of T2 hyperintensity and BPE are associated with false positives [3,9–11]. Although our study did not find a significant difference in terms of BPE and T2 signal, the effect of small tumor size on false-negative results is consistent with the literature.
In patients with a positive family history, the rate of false negatives was found to be significantly high, similar to the study by Avdan Aslan et al. [8]. Although no independent effect was detected in multivariate analysis, it should be considered that the KS alone may not be sufficient in high-risk cases with a family history, and multimodal approaches may be necessary. Detection of local recurrence after modified radical mastectomy may be difficult. A study by Yoo et al. [12] involving 964 breast reconstruction patients showed that 50% of recurrences mimicked the imaging findings of benign lesions. This situation emphasizes the importance of considering clinical risk factors together with radiological evaluation.
In our study, it is noteworthy that ILC was not observed in the false-negative group from a histopathological perspective. The literature indicates that ILC may cause diagnostic difficulties on MRI due to its more diffuse growth pattern [13]. In our cohort, the absence of this histological subtype in the false-negative group may be due to the limited number of patients. HER2 positivity was associated with false negativity in univariate analysis but was not an independent predictor in multivariate analysis. Reviewing the literature, only the study by Avdan Aslan et al. [8] evaluated HER2 status, and no association was found with the KS in that study. In our study, HER2 positivity was associated with a false-negative KS score, and it was thought that this could be due to a heterogeneous contrast pattern.
In recent years, it has been suggested that modifying the KS could reduce false negatives. Integrating ADC values or the presence of microcalcifications into the score may improve diagnostic accuracy [14]. Furthermore, a systematic review and meta-analysis published in 2025 reported that the KS has a higher sensitivity and specificity balance compared to BI-RADS, but emphasized that false negatives remain a limitation in small lesions and specific histopathological subtypes [6]. In the literature, KS stands out as a more objective and systematic decision support tool compared to BI-RADS, increasing diagnostic accuracy in both experienced and inexperienced observers and reducing unnecessary biopsies [2,5]. However, understanding the relationship between false negatives and clinical and imaging parameters is important in revealing the limitations of the method. Only a few studies in the literature have evaluated factors associated with false-negative KS results, making our study significant in this regard.
Study limitations
Limitations of our study include its retrospective design, single-center setting, and low number of false-negative patients. Because the number of false-negative events was limited, multivariable estimates may be unstable with wide CIs and potential overfitting; therefore, ORs should be interpreted cautiously and validated in larger cohorts. The exclusion of NME lesions may limit the generalizability of the study, and future studies should specifically evaluate false-negative predictors in NME cases. However, the findings support the critical role of small tumor size in false-negative KSs and contribute significantly to clinical practice.
Conclusions
The KS is a valuable decision support tool in breast MRI, but it carries a risk of false negatives, especially in small tumors. Therefore, it is recommended to evaluate it in conjunction with clinical risk factors, histopathological features, and additional imaging parameters. Multimodal approaches and larger, prospective studies will address the knowledge gap in this area and further optimize the clinical use of the KS.