Introduction
Rectal cancer accounts for approximately one-third of all colon cancers [1]. In rectal cancer, the five-year survival rate reaches about 90-100% because of improved surgical techniques, increased options in chemoradiotherapy, advancing imaging methods, and rising diagnostic performance [2,3]. Moreover, the prognosis of rectal cancer and treatment planning are based on various factors, including tumor extension, the presence of lymphadenopathy, and the histological grade of the tumor [4,5].
Endoscopy is required for histopathological diagnosis of rectal cancer, whereas it has several limitations in demonstrating the depth of tumoral involvement and adjacent organ invasion. Therefore, magnetic resonance imaging (MRI) is a valuable preoperative imaging modality for the evaluation of local invasion and staging [4,6]. The tumor’s morphological features are precisely depicted on MRI. Moreover, diffusion-weighted imaging (DWI) provides assessment of functional and microstructural characteristics. DWI with quantitative measurements contributes to the prediction of the histopathological properties of the tumor and the prognosis of the patient [4,7,8]. Nevertheless, microcirculation, in addition to the diffusion of water molecules, influences conventional DWI parameters.
Intravoxel incoherent motion DWI (IVIM-DWI) can differentiate water diffusion from microcapillary perfusion. In IVIM-DWI, four parameters can be estimated: the apparent diffusion coefficient (ADC); true diffusion (D), reflecting free water molecule movement in the extracellular space; the pseudo-diffusion coefficient (D*), which shows microcapillary perfusion; and the perfusion fraction (f) [9,10]. Several studies in the literature highlight the importance of IVIM-DWI for the staging of various tumors and estimation of their histological behaviors, as well as the evaluation of treatment response [11–15].
Therefore, we aimed to investigate the role of IVIM-DWI in estimating histological differentiation grade and local invasion (T stage) in rectal non-mucinous adenocarcinoma to predict prognosis and support appropriate treatment planning.
Material and methods
Patients
The institutional ethics committee approved this prospective study. Written informed consent of all patients was obtained. Between July 2018 and May 2019, 39 consecutive patients with non-mucinous rectal adenocarcinoma who were diagnosed by endoscopic biopsy were referred for pre-operative MRI examination. Two patients with cardiac pacemakers and one patient with a femur prosthesis artifact were excluded. A total of 36 patients with non-mucinous rectal adenocarcinoma underwent pre-operative abdominal MRI and IVIM-DWI examination in our study. All patients had a pre-operative endoscopic biopsy.
MRI and IVIM-DWI protocol
All patients underwent MRI on a 1.5-Tesla MRI system (Optima MR450w, GE Healthcare, Milwaukee, USA).
The imaging protocol used for upper abdominal MRI in the study consisted of coronal T2-weighted single-shot fast spin-echo (SS-FSE) (field of view [FOV]: 400 mm, slice thickness: 8 mm, slice gap: 1 mm, repetition time [TR]: 4000 ms, echo time [TE]: 90 ms, matrix: 320 × 224), axial T2-weighted SS-FSE (FOV: 410 mm, slice thickness: 6 mm, slice gap: 1 mm, TR: 4000 ms, TE: 90 ms, matrix: 320 × 224), axial fat-suppressed T2-weighted SS-FSE (FOV: 410 mm, slice thickness: 6 mm, slice gap: 1 mm, TR: 4000 ms, TE: 90 ms, matrix: 320 × 224), axial dynamic pre- and post-contrast T1-weighted three-dimensional (3D) spoiled gradient echo liver acquisition with volume acceleration (LAVA) (FOV: 256 mm, slice thickness: 5.6 mm, TE: 2.1 ms, TR: 6.6 ms, matrix: 256 × 192), post-contrast coronal T1-weighted 3D LAVA (FOV: 430 mm, slice thickness: 5 mm, TE: 2.1 ms, TR: 6 ms, matrix: 320 × 224), and axial DWI sequence (FOV: 410 mm, slice thickness: 6 mm, slice gap: 1 mm, TE: 82 ms, TR: 6000 ms, matrix: 96 × 128, number of excitations: 4).
The imaging protocol used for lower abdominal MRI in the study consisted of sagittal T2-weighted periodically rotated overlapping parallel lines with enhanced reconstruction (PROPELLER) (FOV: 330 mm, slice thickness: 5 mm, slice gap: 1.5 mm, TR: 2643 ms, TE: 90 ms, matrix: 256 × 256), coronal T2-weighted PROPELLER (FOV: 400 mm, slice thickness: 5 mm, slice gap: 1.5 mm, TR: 6115 ms, TE: 71 ms, matrix: 256 × 192), axial T2-weighted fast relaxation fast-recovery fast spin-echo (FR-FSE) (FOV: 430 mm, slice thickness: 5 mm, slice gap: 1.5 mm, TR: 7773 ms, TE: 110 ms, matrix: 256 × 192), axial T1-weighted spin-echo (FOV: 430 mm, slice thickness: 5 mm, slice gap: 1.5 mm, TR: 744 ms, TE: 23.5 ms, matrix: 256 × 192), pre- and post-contrast axial T1-weighted 3D LAVA (FOV: 430 mm, slice thickness: 5 mm, TE: 2.1 ms, TR: 6.6 ms, matrix: 256 × 192), and axial IVIM-DWI sequence (FOV: 380 mm, slice thickness: 5 mm, slice gap: 1 mm, TE: 78 ms, TR: 4000ms, matrix: 80 × 128).
Total scan time for IVIM-DWI was approximately 3-4 min. IVIM-DWI acquisition was performed in the axial plane by applying diffusion-sensitive gradients in all three directions (x, y, z) using a breath-hold single-shot turbo spin-echo echo-planar imaging (SS-TSE-EPI) sequence at 11 different b values (0, 50, 100, 150, 200, 400, 600, 800, 1000, 1200, 1500 s/mm2). Isotropic images consisted of ‘trace’ images obtained by multiplying the signal intensities measured in x, y, and z directions to eliminate direction-dependent signal changes. ADC maps of isotropic images were created automatically.
Among patients who underwent operations (n = 18), abdominal MRI and IVIM-DWI examinations were performed 5 to 7 days before surgery. Patients who received neoadjuvant chemoradiotherapy were scanned at least two months after treatment completion. Because the aim of the study was not to analyze the impact of neoadjuvant treatment on intravoxel incoherent motion (IVIM) parameters, no separate subgroup analysis was performed.
Radiological and histological evaluation
The MRI and IVIM-DWI findings were investigated by two radiologists in consensus before surgery or neoadjuvant treatment. Evaluation and measurements were performed at the workstation (AW Volume Share 7, GE Healthcare, Milwaukee, USA), and IVIM data were processed in the IVIM* (GE Healthcare, Milwaukee, USA) program. The maximum diameter, T1- and T2-weighted signal intensities, contrast enhancement pattern of rectal tumors, presence of lymphadenopathy, involvement of the serosa, adjacent organ involvement, features of lymph nodes (size, shape, contour), and distant metastases were noted.
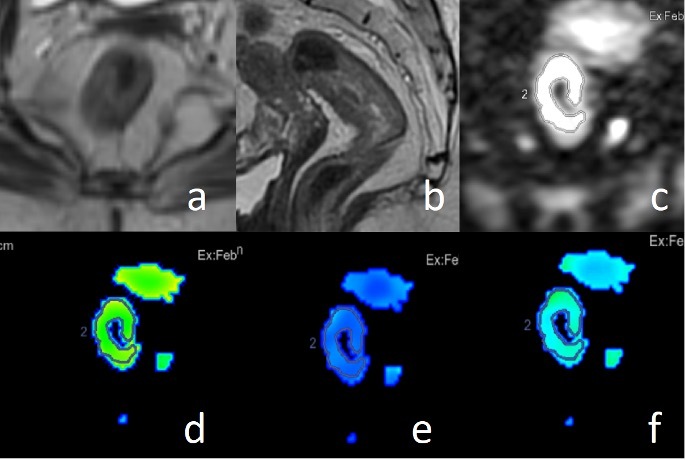
In DWI, three consecutive region of interest (ROI) measurements were performed manually at the widest solid component of the tumor, with exclusion of cystic or necrotic components. The average of these three ROIs was estimated. D, D*, f, and ADC values were calculated from each measurement (Figures 1 and 2).
Figure 1
Axial (A) and sagittal (B) T2-weighted images, diffusion-weighted imaging (DWI) (C), and intravoxel incoherent motion-DWI parameter maps including true diffusion (D), pseudo-diffusion coefficient (E) and perfusion fraction (F) in a patient with rectal cancer
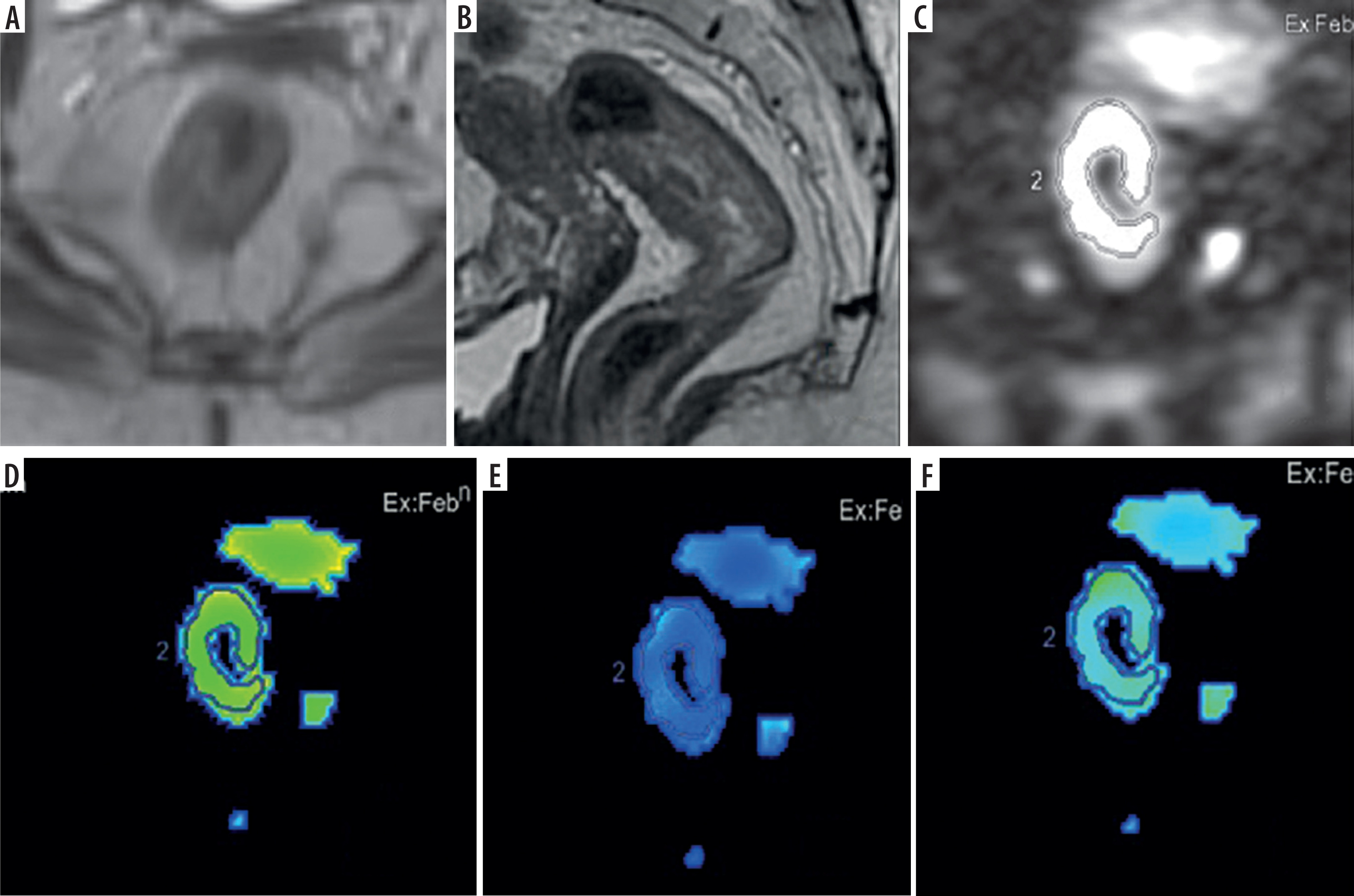
Figure 2
Axial T2-weighted image (A), diffusion-weighted imaging (DWI) (B), apparent diffusion coefficient map (C), and intravoxel incoherent motion-DWI parameter maps including true diffusion (D), pseudo-diffusion coefficient (E) and perfusion fraction (F) of metastatic lymphadenopathy in a patient with rectal cancer
All patients had biopsy-proven non-mucinous rectal adenocarcinoma. In patients who underwent surgical resection, the reference standard was surgical histopathology for evaluation of tumoral invasion and lymph node metastasis. In clinically inoperable patients demonstrating adjacent organ invasion on imaging, conventional MRI served as the reference standard for T4 staging and invasion assessment. Patients were classified according to histological differentiation, tumoral invasion depth, and the presence of pathological lymph nodes, based on histopathological results and conventional MRI. The comparison of histopathological results and MRI findings with IVIM-DWI parameters was analyzed statistically. Lymph node evaluation was performed using a lesion-based approach; each lymph node was analyzed individually and treated as a separate data point regardless of the number of nodes present within the same patient. Nonetheless, metastatic lymph node categorization was performed only in surgical patients. In patients with no malignant lymph nodes in the pathological specimen, lymph nodes > 0.5 cm on conventional MRI were considered benign. A malignant lymph node group was formed based on histopathological verification and the demonstration of metastatic lymph nodes on conventional MRI.
Statistical analysis
Statistical analyses were conducted using the Number Cruncher Statistical System 2007 software (Kaysville, Utah, USA). Descriptive statistical methods (mean, standard deviation, median, frequency, ratio, minimum, maximum) were employed to evaluate the study data, and the distribution of the data was assessed using the Shapiro-Wilk test. The Mann-Whitney U and Kruskal-Wallis tests were used to compare quantitative data between groups. Receiver operating characteristic (ROC) analysis was performed to identify the predictive values. The p-level < 0.05 was considered statistically significant.
Results
A total of 36 patients, composed of 20 men (56%) and 16 women (44%), were included in this study. The mean age was 61 ± 8 years (range: 28-85 years).
Evaluation of IVIM-DWI parameters according to histological differentiation grade
All patients had biopsy-proven rectal non-mucinous adenocarcinoma with a known histological differentiation grade. The patients were classified into three groups according to histological differentiation: eight (22%) were poorly differentiated, 22 (61%) were moderately differentiated, and six (17%) were well differentiated. In comparison of IVIM parameters of rectal adenocarcinomas with known differentiation grades, a lower f value was achieved in the higher histological grade (p < 0.01). The mean f value in well-, moderately and poorly differentiated tumors was 31.86, 23.79, and 19.96, respectively (Table 1).
Table 1
Statistical results of intravoxel incoherent motion parameters according to histological differentiation
| Parameter | Well differentiated | Moderately differentiated | Poorly differentiated | p* |
|---|---|---|---|---|
| D (× 10−3 mm2/s) | 1.169 ± 0.27 | 1.047 ± 0.19 | 1.139 ± 0.29 | 0.823 |
| D* (× 10−3 mm2/s) | 11.31 ± 2.36 | 12.00 ± 4.77 | 12.62 ± 4.18 | 0.294 |
| f (%) | 31.86 ± 7.24 | 23.79 ± 4.78 | 19.96 ± 8.42 | 0.006 |
| ADC (b = 1000 mm2/s) (× 10−3 mm2/s) | 1.55 ± 0.31 | 1.33 ± 0.27 | 1.34 ± 0.33 | 0.373 |
| ADC (b = 1500 mm2/s) (× 10−3 mm2/s) | 1.36 ± 0.28 | 1.17 ± 0.27 | 1.22 ± 0.32 | 0.577 |
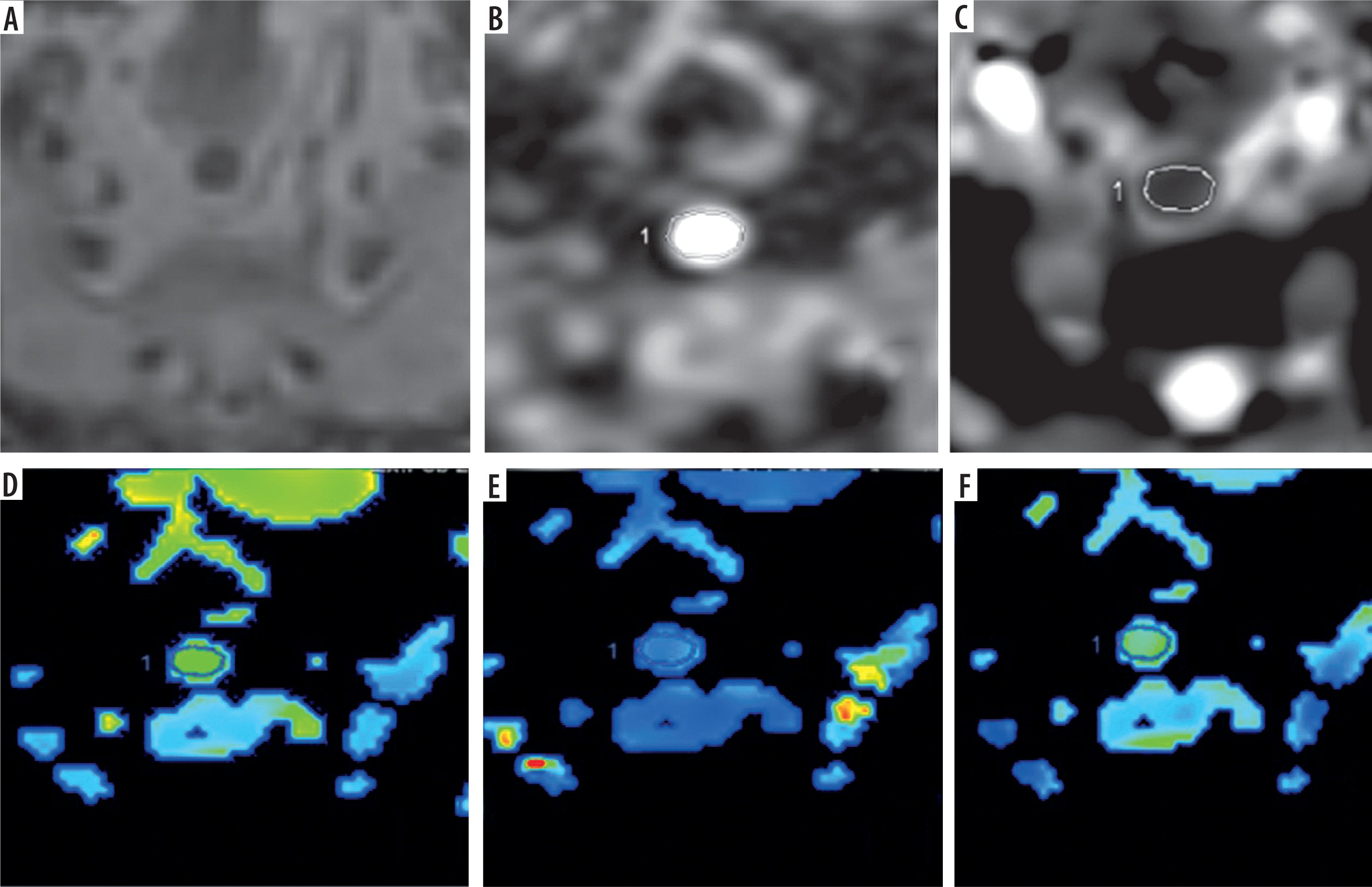
In differential diagnosis of well- and moderately differentiated tumors, the optimal cut-off value for the f parameter was 30, with 67% sensitivity, 100% specificity, positive predictive value of 64%, and negative predictive value of 96 (area under the curve [AUC]: 0.802 ± 0.125, p < 0.05) (Figure 3), whereas in differentiation of poorly differentiated tumors from well- and moderately differentiated tumors, the cut-off value of < 20.89 showed 88.5% sensitivity and 85.7% specificity (AUC: 0.771, p < 0.05).
Contribution of IVIM-DWI parameters to detection of adjacent organ invasion
In surgical patients (n = 18), the invasion degree was assessed from the surgical specimen. In the non-surgical patients, conventional MRI findings were evaluated by two radiologists, and adjacent organ invasion or peritoneal involvement was noted in nine patients. Among these patients, bladder (n = 4), prostate (n = 2), seminal vesicle (n = 1), uterus (n = 1), and adjacent peritoneum (n = 1) invasions were observed.
Among 27 patients, four had submucosal invasion (T1), two had muscularis propria invasion (T2), 11 had serosal and perirectal fatty tissue invasion (T3), and 10 had peritoneal or adjacent organ invasion (T4). T1 and T2 tumors formed early-stage tumors, and T3 and T4 tumors formed late-stage tumors (Table 2). In comparison of early-stage (T1-T2) and late-stage (T3-T4) tumors with respect to IVIM parameters, late-stage tumors showed significantly lower D, D*, and ADC values (p < 0.05) (Table 3). The ROC analysis results for IVIM parameters in the differential diagnosis of early and late-stage tumors are shown in Table 4.
Table 2
Distribution of patients according to local invasion degrees
Table 3
Comparison of intravoxel incoherent motion (IVIM) diffusion-weighted imaging parameters between early and late stage rectal cancers
| IVIM parameter | Early stage (T1-T2) | Late stage (T3-T4) | p* |
|---|---|---|---|
| D (× 10−3 mm2/s) | 1.344 ± 0.294 | 1.001 ± 0.232 | 0.013 |
| D* (× 10−3 mm2/s) f (%) | 14.719 ± 3.430 | 10.97 ± 3.150 | 0.011 |
| 26.26 ± 11.99 | 24.39 ± 5.81 | 0.929 | |
| ADC (× 10−3 mm2/s) (b = 1000 mm2/s) | 1.660 ± 0.215 | 1.273 ± 0.241 | 0.007 |
| ADC (× 10−3 mm2/s) (b = 1500 mm2/s) | 1.491 ± 0.196 | 1.137 ± 0.220 | 0.016 |
Table 4
Receiver operating characteristic analysis results for intravoxel incoherent motion (IVIM) parameters in differential diagnosis of early- and late-stage tumors
| IVIM parameter | Cut-off value (× 10−3 mm2/s) | Sensitivity (%) | Specificity (%) | AUC ± SD (95% CI)a | p* |
|---|---|---|---|---|---|
| D value | 1.17 | 83.3 | 80 | 0.833 ±0.088 (0.660-0.981) | 0.015 |
| D* value | 13.71 | 85 | 83.3 | 0.842 ±0.137 (0.573-0.964) | 0.013 |
| ADC value (b = 1000 mm2/s) | 1.433 | 92 | 75 | 0.858 ±0.085 (0.712-0.993) | 0.009 |
| ADC value (b = 1500 mm2/s) | 1.132 | 83 | 70 | 0.825 ±0.084 (0.661-0.989) | 0.018 |
Assessment of IVIM parameters in differentiation of metastatic from non-metastatic lymph nodes
In surgical patients (n = 18), metastatic lymph nodes were detected in eight patients. The remaining 10 patients had non-metastatic lymph nodes. In patients with metastatic lymph nodes (n = 8), a total of 24 metastatic lymph nodes were identified in the surgical specimens. These metastatic lymph nodes were retrospectively evaluated on conventional MRI according to their location described in the histopathological report. In patients with non-metastatic lymph nodes, the lymph nodes greater than 0.5 mm were also retrospectively reviewed on conventional MRI. Subsequently, a total of 43 (metastatic [n = 24, 56%] and non-metastatic [n = 19, 44%]) lymph nodes were analyzed retrospectively.
In metastatic lymph nodes, D, D*, and ADC values were lower than those of non-metastatic ones (p < 0.05) (Table 5). The ROC analysis and optimal cut-off values of IVIM parameters in the differentiation of metastatic from non-metastatic lymph nodes are shown in Table 6.
Table 5
Comparison of intravoxel incoherent motion diffusion-weighted imaging parameters between metastatic and non-metastatic lymph nodes
| Parameter | Metastatic lymph nodes | Non-metastatic lymph nodes | p* |
|---|---|---|---|
| D (× 10−3 mm2/s) | 0.743 ± 0.112 | 1.017 ± 0.286 | 0.001 |
| D* (×10−3 mm2/s) | 10.62 ± 4.68 | 21.37 ± 13.86 | 0.001 |
| f (%) | 33.20 ± 11.44 | 26.99 ± 8.71 | 0.055 |
| ADC (× 10−3 mm2/s) (b = 1000 mm2/s) | 1.123 ± 0.252 | 1.399 ± 0.358 | 0.016 |
| ADC (× 10−3 mm2/s) (b = 1500 mm2/s) | 0.935 ± 0.221 | 1.199 ± 0.381 | 0.008 |
Table 6
Receiver operating characteristic analysis and cut-off values of intravoxel incoherent motion (IVIM) parameters in differentiation of metastatic from non-metastatic lymph nodes
| IVIM parameters | Cut-off value (× 10−3 mm2/s) | Sensitivity (%) | Specificity (%) | AUC ± SD (95% CI)a | p* |
|---|---|---|---|---|---|
| D value | 0.936 | 74 | 96 | 0.795 ± 0.071 (0.662-0.928) | 0.001 |
| D* value | 12.7 | 74 | 83 | 0.827 ± 0.064 (0.704-0.950) | 0.001 |
| ADC value (b = 1000 mm2/s) | 1.205 | 70 | 73 | 0.680 ± 0.084 (0.521-0.839) | 0.016 |
| ADC value (b = 1500 mm2/s) | 1.07 | 73 | 88 | 0.739 ± 0.079 (0.591-0.887) | 0.008 |
Discussion
Pre-operative imaging is essential for appropriate treatment planning in patients with rectal carcinoma. In routine abdominal MRI, tumoral involvement, the presence of lymphadenopathy, and adjacent organ invasion can be precisely detected [16–19]. However, advances in technology have enabled functional MRI to provide quantitative insights into tumor microstructure beyond morphological characteristics. DWI has made constructive contributions to the depiction of biological behavior in different cancer types [20–22]. Therefore, the influence of IVIM-DWI parameters in the staging of rectal carcinoma and the determination of tumoral aggressiveness was analyzed in our study. Moreover, a significant relationship was found between histopathological findings and IVIM-DWI parameters.
Our study focused on the relationship between histopathological differentiation and perfusion fraction. Higher f values were obtained in well- and moderately differentiated tumors than in poorly differentiated tumors. The f value, as an indicator of microcapillary circulation, reveals tumoral aggressiveness and growth potential. Well- and moderately differentiated tumors have more regular microvascular structures, which are associated with higher f values; in poorly differentiated tumors, a greater tumoral growth rate results in insufficient microcapillary development, leading to lower f values. Lu et al. [23] reported a negative relationship between tumoral differentiation and f value. In a previous study, lower f values in poorly differentiated tumors were associated with inadequate microvascular development [24]. Sun et al. [25] reported that poorly differentiated tumors showed lower f, D*, and ADC values. Our results align with previous studies and demonstrate that the f value can provide information about tumoral differentiation. In addition, our findings suggest that the perfusion fraction may contribute to preoperative risk stratification, as higher f values reflect a more preserved tumor microvasculature, characteristic of better-differentiated lesions.
In evaluating the relationship between tumor extension and IVIM parameters, late-stage (T3-T4) tumors compared to early-stage (T1-T2) tumors had lower D, D*, and ADC values, indicating decreased diffusion due to tumoral hypercellularity. In our study, among IVIM parameters and ADC values, sensitivity, specificity, and diagnostic performance were highest with the mono-exponential model at b values of 0 and 1000 s/mm2. A previous study investigated the relationship between tumoral invasion and IVIM parameters. It revealed that lower D and D* parameters were related to increasing tumoral stages [25]. A similar study reported that D, D*, and ADC parameters are negatively correlated with tumoral invasion degree [24]. Moreover, other previous studies have shown that a higher invasion degree of rectal cancer showed lower ADC values [26–28]. One study showed that the ADC map achieved by b = 1000 s/mm2 achieved the best diagnostic performance in detecting the relationship between tumoral invasion and ADC values [29]. Similarly, our results for the ADC map at b = 1000 s/mm2 are consistent with the literature. These results reinforce previous observations and indicate that both ADC (b = 1000 s/mm2) and D values may serve as useful biomarkers in differentiating early- and late-stage rectal carcinoma.
The determination of metastatic lymph nodes has an important role in the staging of rectal cancer. In our study, metastatic lymph nodes had significantly lower D, D*, and ADC values compared to non-metastatic lymph nodes. This finding supports the hypothesis that tumoral cellularity restricts diffusion in both the primary tumor and metastatic lymph nodes. Yu et al. [30] demonstrated that lower D and D* values were obtained in metastatic lymph nodes. Additionally, in the literature, most studies on metastatic lymph nodes across different malignancies reported lower ADC values [31–33]. Taken together, these findings suggest that IVIM-derived parameters may complement conventional MRI for nodal stratification, especially when radiological criteria alone are insufficient.
This prospective study has some limitations. A small sample size was one of them. Additionally, in patients who received neoadjuvant chemotherapy but did not undergo surgery, IVIM parameters may still be influenced by residual treatment-related alterations in perfusion and diffusion characteristics, even if imaging is performed after a standard waiting period. Since the present work was not designed to assess the impact of neoadjuvant therapy on IVIM metrics, no dedicated subgroup analysis was performed. Moreover, in clinically inoperable T4 patients, staging and invasion assessment relied on conventional MRI rather than histopathology, potentially introducing classification bias. Another limitation is that lymph node analysis was performed at the lesion rather than the patient level, which may introduce intra-patient clustering effects in cases with multiple lymph nodes originating from the same subject. Finally, IVIM measurements were performed by consensus readings, and interobserver variability was not evaluated; therefore, potential observer-dependent differences could not be assessed. Further prospective studies with large populations are recommended.
In conclusion, aggressive tumors with low histological differentiation and metastatic lymphadenopathy exhibit lower diffusion and perfusion values. As a perfusion indicator, the f value provides valuable findings about tumoral differentiation. IVIM-DWI can be used as an adjunctive modality to routine abdominal MRI in the pre-operative assessment of rectal non-mucinous adenocarcinoma.